Our long history of ignoring diseases that emerge in Africa as solely of concern to the African continent has been proven wrong time and time again, but yet, we still haven’t learned. We must gain an appreciation for how interconnected the world is today. The CDC has already acknowledged that Marburg virus has spread to other parts of the world through international travel. https://www.cdc.gov/marburg/outbreaks/index.html.
I remember well, when a similar disease caused by Ebola virus that was seemingly isolated to Africa, presented to a hospital in Dallas, Texas in September of 2014 in a traveler from Liberia. Two nurses at that Dallas hospital were exposed to the patient and came down with Ebola virus disease. Fortunately, despite the high mortality rate, both nurses survived.
Marburg virus was first detected in 1967 through simultaneous outbreaks in laboratories working with African green monkeys imported from Uganda in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia. In addition to the 31 reported cases, an additional primary case was later diagnosed by blood test. There were 31 cases and 7 deaths (23 percent fatality rate).
In 1975, a man with a recent travel history to Zimbabwe was admitted to a hospital in South Africa. Infection spread from the man to his traveling companion and a nurse at the hospital. The man died, but both women eventually recovered (33 percent fatality rate).
In 1980, a patient who had recently traveled to Kenya was hospitalized with Marburg virus disease in Nairobi and subsequently died. A doctor who attempted to revive the patient developed symptoms nine days later but recovered. There were two cases and one death (50 percent fatality rate).
In 1987, a 15-year-old Danish boy was hospitalized with a 3-day history of headache, malaise, fever, and vomiting. Nine days prior to symptom onset, he had visited Kitum Cave in Mount Elgon National Park in Kenya. Despite aggressive supportive therapy, the patient died on the 11th day of illness. No further cases were detected. (100 percent fatality rate).
There was a large outbreak of Marburg virus disease between 1998 and 2000. Most cases occurred in young male workers at a gold mine in Durba, in the northeastern part of the Democratic Republic of Congo, which proved to be the epicenter of the outbreak. Cases were later detected in the neighboring village of Watsa. There were 154 cases and 128 deaths (83 percent fatality rate).
Between 2004 and 2005, an outbreak of Marburg virus disease is believed to have begun in Uige Province in Angola in October of 2004. Most cases detected in other provinces have been linked directly to the outbreak in Uige. There were 252 cases and 227 deaths (90 percent fatality rate).
In 2007, there was a small outbreak, with four cases in young males working in a lead and gold mine in Uganda. To date, there have been no additional cases identified. There was one death (25 percent fatality rate).
In 2008, a U.S traveler returned from Uganda in January 2008, became ill and fortunately survived. A diagnosis of Marburg virus disease was confirmed.
Also in 2008, a 40-year-old Dutch woman with a recent history of travel to Uganda was admitted to hospital in the Netherlands. She had visited a cave in Maramagambo forest in Uganda, at the southern edge of Queen Elizabeth National Park. Three days before hospitalization, the first symptoms (fever, chills) occurred, followed by a rapid deterioration in her health. The woman died on the 10th day of the illness (100% fatality rate).
In 2012, testing at CDC/UVRI identified a Marburg virus disease outbreak in the districts of Kabale, Ibanda, Mbarara, and Kampala in Uganda over a 3-week period. There were 15 cases and 4 deaths (27 percent fatality rate).
In 2014, one case was confirmed (fatal) and 197 contacts were followed for 21 days. Out of these 197 contacts, eight developed symptoms similar to Marburg, but all tested negative at the Uganda Virus Research Institute (UVRI) with support from CDC (100 percent fatality rate).
In 2017, a blood sample from Kween District in Eastern Uganda tested positive for Marburg virus. Within 24 hours of confirmation, a rapid outbreak response was begun. This outbreak occurred as a family cluster with no additional transmission outside of the four related cases. There were four cases and three deaths (75 percent fatality rate).
In 2021, in Guinea, one case was reported and confirmed by the Guinean Ministry of Health in a patient who was diagnosed after death. No additional cases were confirmed after more than 170 high-risk contacts were monitored for 21 days (100 percent fatality rate).
In 2022, a fatal case of Marburg disease was identified in the Ashanti region of Ghana on July 7, 2022. Marburg disease was initially detected through testing at Ghana’s national laboratory marking the first detection of Marburg disease in Ghana. Shortly after, two additional family members were also confirmed to have Marburg disease. No additional cases outside the family cluster were identified. The outbreak was declared over in September. There were three cases and 2 deaths (67 percent fatality rate).
And, now, for the first time involving this country, there is a large outbreak in Rwanda. There have already been 27 cases identified, but sadly nine of them have died. Disturbingly, more than 70 percent of these cases are in health care workers who work at either of two hospitals in the capital city of Rwanda – Kigali (population 1.7 million people). That suggests to me that the health care workers were likely exposed to Marburg virus by patients in whom the diagnosis was missed, and thus, there may be many more cases in the community. In addition, three hundred close contacts are being monitored for signs or symptoms of the disease.
The other concern is that Kigali is the home to both a regional and international airport with destinations to nearly 20 countries, including in the Middle East and Asia.
Marburg virus causes rare, but deadly infections in humans, of the hemorrhagic fever type. Marburg virus can also infect primates. Symptom onset is often sudden and can consist of fever, rash (often on the chest, back and abdomen) and severe bleeding. The natural host for Marburg virus is the Egyptian rousette bat (Rousettus aegyptiacus) and bats can then transmit the infection to people, i.e., this is a zoonotic infection. The incubation period ranges from 2 – 21 days.
The infection spills over from infected bats to humans through bat saliva, urine or feces. An infected person may then transmit the infection to a close contact who comes in contact with the infected person’s secretions or body fluids (including in the postmortem period) or contact with fomites (bedding, clothing, needles, or medical equipment used by the patient). As has been documented for the Ebola virus, Marburg virus may persist in the testes of recovered male patients and then be transmitted through sex even after the male’s recovery.
Despite the repeated outbreaks over nearly sixty years, the severity of the disease, the risk to health care workers, the emergence of infection in new African countries, and now the assessment by the World Health Organization that the risk for spread to neighboring countries is high and the acknowledgement of the risk of spread beyond East Africa (specifically, national level – high; regional level – high; global level – low), there are no approved treatments or vaccines for this disease.
This occurs at the same time that the WHO has declared a Public Health Emergency of International Concern due to an outbreak of monkeypox clade Ib virus and Mpox cases in Africa that is affecting some of Rwanda’s neighboring countries. Rwanda itself has had 4 confirmed cases as of the last update I could find from almost two weeks ago. Monkeypox clade IIb already caused a global outbreak in 2022.
Hopefully, we will devote some funding to better understanding the biology of this virus, investigating antiviral treatments, and developing vaccines. We should have learned that it is far easier and far less expensive to contain outbreaks than to respond to them on a global level.
Surveillance and Containment of Novel Infectious Agents with Pandemic Potential – We are Not Good at This
The old saying, “An ounce of prevention is worth a pound of cure,” is no more apt than in the field of global outbreaks and pandemics. In other words, the cost of responding aggressively to novel infectious agents with pandemic potential, even if they ultimately do not cause an epidemic or pandemic is far less costly (in terms of dollars, societal costs and health care costs) than if we respond lethargically and allow the infection to spread among animals and eventually to humans and beyond the initial geographic borders before we decide to get serious about it. We need only look the past two years at our non-response to Mpox outbreaks in Africa over decades that ultimately became a Public Health Emergency of International Concern with global spread in 2022. You would think “well, surely we learned our lesson from that,” but now two years later, we are faced with a second Public Health Emergency of International Concern with another outbreak in Africa with yet a different strain of Mpox that is now showing up in countries that have never had cases of Mpox before and appears to potentially cause higher morbidity and mortality, and unlike the strain involved in 2022 that appeared to be largely spreading among communities of men who have sex with men, this one appears to infect a much broader range, including children and heterosexual adults.
In addition to early interventions being cost-effective and potentially sparing many lives, just undergoing a systematic epidemiological investigation, as well as studies of the infectious agent and its biological properties, receptor affinities, mode of transmission, and pathogenesis (the mechanisms by which it produces disease) as well as studies of the immune response of those who are infected and potential vaccines or therapies, would generate tremendously valuable information about the specific infectious agent, but also potentially add to our knowledge about related infectious agents (e.g., our studies and knowledge of smallpox have accelerated our knowledge and vaccine options against monkeypox) and contribute to our general understanding of bacteria, viruses, fungi, prions, or whatever the infectious threat turns out to be.
Now, for at least the third time, in just two years, we appear to be making all the same mistakes and omissions again as we are faced with a new strain of avian influenza virus that is spreading largely uncontrolled among U.S. dairy farms.
In late 2000, when my soon-to-be coauthor contacted me about the idea of writing a book, after my wife had already planted that idea in my head six months earlier, I became convinced that there was a need for us to write that book (Preparing for the Next Global Outbreak: Lessons from the Schoolhouse to the White House), because it was already becoming clear to me that we were making many mistakes and appeared not to be learning from these. That book was the opportunity for us to chronicle our learnings from the COVID-19 pandemic and to capture the learnings, as well as laying out 117 specific recommendations with the hopes that the next time we were threatened with a global outbreak, hopefully it would be unnecessary to repeat all these mistakes.
An article was published in Nature two days ago in which some influenza experts offered a review and their perspective on the global H5N1 (this is the scientific reference to a particular avian influenza [bird flu] virus) influenza panzootic (this is the term for a pandemic in animals) in mammals The global H5N1 influenza panzootic in mammals | Nature. I think this will be of interest to readers on my blog, so I will summarize it below:
In their introduction, they call out a point that I have made a number of times on the radio show I appear on weekly (Idaho Matters with Gemma Gaudette, Boise State Public Radio https://www.npr.org/podcasts/605235114/idaho-matters): Influenza A (this group includes some human seasonal influenza viruses, as well as avian influenza viruses) has been responsible for more pandemics among humans than any other organism in history to our knowledge, but definitely in the past century. Thus, any outbreak of influenza A among humans or animals deserves our attention, at the very least.
While generally we think of avian influenza viruses as causing infections in waterfowl and wild birds that then contaminate feed or feeding grounds and infect domestic birds, especially poultry, the current global outbreak is different and concerning due to: (1) the rapid global spread of the virus including to South America and Antarctica for the first time; (2) the rapid evolution and changes to the virus resulting from reassortment (this is a process characteristic of influenza viruses whose genetic material largely consists of 8 segments, of which one or more can be easily swapped with another influenza virus when a human or other animal is infected with, for example, one avian influenza virus and one human influenza virus, resulting in a significant change in the virus that can lead to adaptation of the avian virus to better infect mammals, which otherwise the avian influenza virus is quite limited in its ability to do), and (3) the frequent spillover to land and marine mammals, many of which we have never detected H5N1 infections in before.
For the first time in the decades that we have been aware of the virus, the H5N1 virus has demonstrated sustained mammal-to-mammal transmission among very diverse species, including most recently (first detected in March of this year) outbreaks among dairy cattle farms in a growing number of herds in a growing number of states in the U.S.
All of these factors should be increasing our assessment of risk for spillover to humans (and we have now detected 15 such cases in the U.S., with concern that there could be many more undetected cases) and the potential (even though currently thought to be low) for this virus to develop the potential to cause a human pandemic.
In the past, with one notable exception (see below) avian influenza viruses have caused human pandemics, but only after first infecting swine that served as the “mixing bowl” for reassortment of the avian influenza virus with other influenza A viruses that gave the avian influenza virus the ability to efficiently infect humans and the ability for efficient human-to-human transmission. These authors lay out information that we have learned that raises the potential that the currently uncontrolled spread of the virus in other mammals, particularly dairy cows, may serve the “mixing bowl” function that swine have done in the past.
The authors include the graphic below to demonstrate how the H5N1 highly pathogenic avian influenza A virus has spread from being isolated to Asia to encompassing the United States within 15 years, and several years later, throughout much of the world.
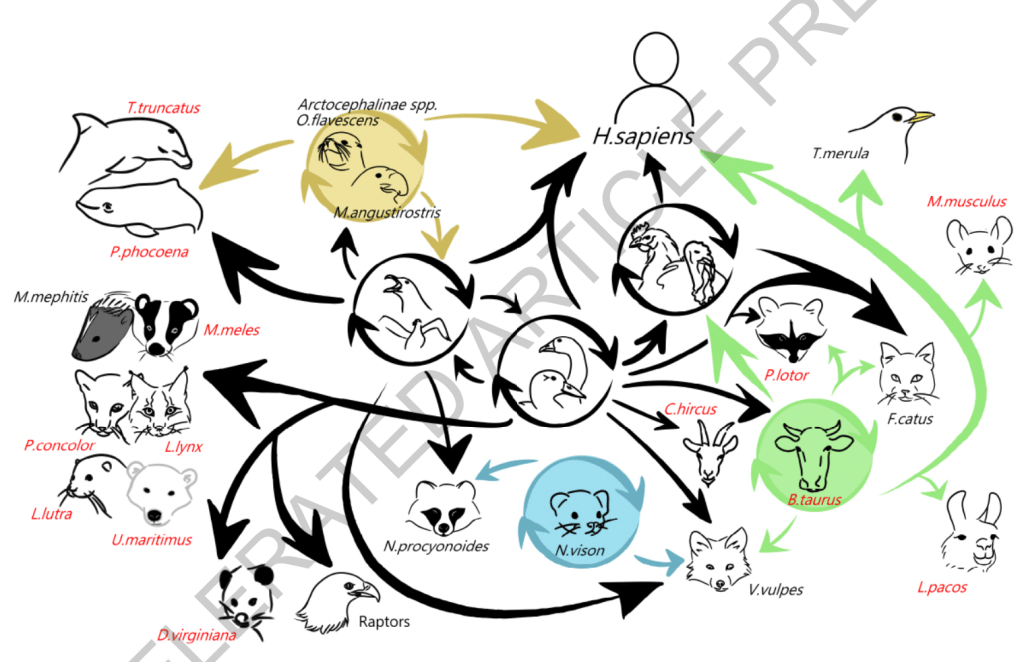
This next graphic depicts the range of mammalian species that have been infected by the virus, most of these for the first time in the virus’ history to our knowledge:
We need to keep in mind that spread of the virus to and among a greater number of mammals presents the virus with many more opportunities to evolve in ways that increase transmissibility and that equip the virus with more defenses against mammalian immune responses. Both of these, in turn, increase the threat of more efficient spread to humans, and ultimately could result in more efficient transmission among humans, the final step between this remaining a panzoonotic event and becoming a human pandemic.
The authors point out that the change in threat level occurred in 2020 when a new genotype (genetic form of the virus) developed that is referred to as clade 2.3.4.4b (you can think of clade as another word for strain). That lead to greater spread around the world and greater spread to a wider range of animals.
In the past, when a different avian influenza virus spread to the U.S. from Asia, outbreaks were contained with surveillance and culling of infected poultry. This time is different. Culling of infected poultry has not stopped the spread of this virus and now, for the first time, outbreaks are occurring on an increasing number of dairy farms in a growing number of states. It appears that wild migratory birds are continuing to introduce the virus on dairy and poultry farms as they fly over, including during migration.
The current clade spreading among dairy cattle in the U.S. is the clade 2.3.4.4b – the result of the virus having undergone a number of reassortments (swapping of segments of the genetic material with other influenza viruses the host was infected with) – going back to a reassortment between an H5N8 avian influenza virus and a Eurasian low pathogenic avian influenza virus.
Initially, there was a single spillover event of the H5N1 virus from wild birds to U.S. dairy cattle (in Texas), likely in late 2023 or early 2024, after which there was onward transmission from cattle to other cattle likely through virus on milking machines, though the contribution of respiratory transmission remains unclear. There was subsequent spread to other dairy farms by transport of infected cattle, as well as spillover events from cattle to other animals and wildlife, most notably cats that drank raw milk spillage on these farms.
The authors then pose and try to answer the critical question: Could this virus spark a pandemic?
The authors point out that for an influenza virus to spark a pandemic, it must fulfill two key criteria. First, the main attachment protein of the virus (i.e., hemagglutinin, from which each virus is given the “H” designation – in this case, H5) must be antigenically novel (meaning that the immune systems of a sufficiently large portion of the population have not previously been exposed to it and would not be able to recall prior immune memory to make a rapid antibody response). This criterion is fulfilled, as human seasonal influenza viruses are of the H1 or H3 type, predominantly. H5 has never before circulated in humans, and thus, it would be antigenically novel, and further, there is no evidence to support that humans would have cross reactive immunity from any of our past hemagglutinin protein exposures.
The second criterion is a much higher, but not impossible, bar to meet: efficient transmission between humans.
Based on our current understanding, we believe that would require three changes to an avian influenza virus (and these would most likely occur through the reassortment process). The first change is in the viral polymerase (PB2, PB1, and PA proteins) that helps the virus exploit mammalian host machinery to replicate (make the viral proteins necessary to assemble new virions) by way of enabling the avian viral protein able to work with and direct the human cellular components it needs for the process of protein synthesis. A second change must occur in the hemagglutinin protein (remember, this gives the influenza virus its H designation) to help the virus bind strongly to cell surface receptors abundant in the human upper respiratory tract (URT) since avian influenza viruses preferentially use cell receptors with α 2, 3 -sialic acids attached to their cell surface glycoproteins, whereas humans do not generally have this configuration in the upper respiratory tract (rather, we have α 2, 6 -sialic acids on our cell surface glycoproteins). This is critical because levels of virus are highest in respiratory secretions and aerosols when the virus is present in the upper respiratory tract of the person emitting the secretions and aerosols. The third change must stabilize the hemagglutinin protein to tolerate lower pH (a more acidic environment) to prevent destruction of the virus when transiting between hosts through the air. For H5N1 viruses, the highest hurdle appears to be the second criterion. The virus’ polymerase is more prone to adaptation than is the ability for the virus to change receptor affinities.
In 1957, this trifecta occurred during dual infection of an individual animal — probably a human, but possibly another species, such as a pig — with an avian H2N2 influenza virus and a human H1N1 influenza virus that resulted in the emergence of a new influenza virus containing the hemagglutinin, the neuraminidase, and the gene for one of the polymerase proteins (PB1) from the avian virus, along with the remaining five genetic segments from the human H1N1 influenza virus, and it sparked a pandemic.
The remnants of that reassortment H2N2 pandemic virus circulated in humans until 1968, when it was replaced by another reassortment virus, the H3N2 Hong Kong virus — created by the replacement of the hemagglutinin (H2) and polymerase (PB1) genes of the H2N2 virus with two new avian genes, H3 and a new PB1 that triggered another pandemic. The Origins of Pandemic Influenza — Lessons from the 1918 Virus | New England Journal of Medicine (nejm.org)
However, while much less common, and perhaps only a once-in-a-century or longer event, we should keep in mind that the most deadly pandemic (in terms of American deaths on a per capita basis) since the late twentieth century was the influenza pandemic of 1917 -1918 (the COVID-19 pandemic killed a greater number of Americans, however, in 1917-1918, the U.S. population was roughly a third of what it is now, so on a per capita basis, the U.S. mortality rate was higher for the influenza pandemic) was caused by an H1N1 virus for which there is no evidence of reassortment, meaning that this avian virus most likely infected humans and then evolved within humans to acquire these necessary mutations and enhanced transmission.
I am concerned that we have uncontrolled spread of the H5N1 virus among dairy cattle. As we approach our seasonal influenza season, will those working on dairy farms transmit our seasonal virus to these animals, where we know that coinfection can occur in cow utters, and will this potentially serve as the “mixing bowl” to allow mutations and reassortments necessary for the three criteria above to be met?
But while this is a concern yet to materialize, there is already a concerning development that further demonstrates how bad we are at surveillance and containment of novel infectious agents with pandemic potential beyond the fact that thus far, six months later, we still are unable to prevent further spread of H5N1 to more dairy farms in more states (the latest being California). This development gives rise to concern that perhaps the second criterion is becoming closer to being met, while public health and agriculture agencies have largely been mounting a response without any sense of urgency, and in some respects, without any sense.
Here is what happened. An individual in Missouri, with a number of underlying health problems, was hospitalized on August 22 of this year. On September 6, the CDC announced that this person was confirmed to have an avian influenza (H5 – reportedly the sample was inadequate to allow for identification of the neuraminidase “N” component) that was detected through the state’s seasonal flu surveillance system. The patient was treated with antiviral therapy and was able to be discharged from the hospital and has since recovered. This was the 14th case of H5 infection in a human in the U.S. in 2024 (15th case in total – there was a case in Colorado in 2022 in a worker involved in culling infected poultry birds). What was particularly concerning about this case was that the person, unlike all the other reported cases, had no occupational exposure to poultry or dairy cows. https://www.cdc.gov/media/releases/2024/s0906-birdflu-case-missouri.html.
The significance of lack of exposure history is the concern for whether the patient was infected through community spread of infection – a clear concern that the second criterion that we discussed above may have been met unbeknownst to us. At that point in time, I was hoping that the patient had ingested raw milk, and it seemed an obvious oversight that the CDC didn’t state whether the patient did so in the announcement. It was not until later that the CDC would confirm that the patient had not ingested raw (unpasteurized) dairy products.
Since then, information has been slow to be updated and has dripped in in an ever-increasingly concerning manner, despite the reassurances from public health agencies that the risk to the public remains low. One week later it was disclosed that a “close contact” was also sick at around the same time as this patient. That person was not tested for influenza. In perplexing statements, the CDC stated that it did not believe that there had been spread of H5N1 between the infected patient and any close contact, without offering any basis for that somewhat surprising statement. “There is no epidemiological evidence at this time to support person-to-person transmission of H5N1 though public health authorities continue to explore how the H5N1-positive individual in Missouri contracted the virus.”
Let me explain why this feels like gas-lighting to those of us not privy to all the information that the CDC has about this case, and can only go on the basis of the drips of information made public. So first let me acknowledge that the investigation is disjointed in that the state has original jurisdiction and the CDC can only insert itself to the extent it is invited by the state. Further, I acknowledge that if we had all the information that the state investigators and CDC have, perhaps I would come to the same conclusion that they have. But, with the limited amount of information that has been made public, the CDC’s statements make no sense. First of all, they state that “there is no epidemiological evidence” to support person-to-person transmission. Well, one key tool of an epidemiological investigation is to do contact tracing. They state that a “close contact” was also sick around the same time as the patient, but was not tested for influenza. So, that is concerning evidence. It is not proof, by any means, but we are being told that someone who was in close contact with the patient was also sick, but we don’t know what illness they had because they were not tested and we don’t know the nature of the close contact. That raises four possibilities: (1) Close contact infected patient; (2) patient infected close contact: (3) patient and close contact were infected by a common unidentified source; or (4) patient had avian influenza infection, but close contact has a contemporaneous, but different and unrelated illness. Despite having no answers, these are not unanswerable questions. The fourth possibility is the most important to answer, and the way you answer that in someone who is no longer sick and therefore cannot be tested with our influenza tests that we use on sick patients is to do a serological test, i.e., we check the person for antibodies to H5N1 in their blood. In response to questioning about this, we are told that the public health authorities were contemplating such testing. (You have to read this next sentence as if I am yelling it, because I was in my head). Contemplating it, good heavens, it takes me 5 minutes to contemplate that kind of testing in my medical practice! All you need is a tourniquet, gloves, a specimen tube, an alcohol swab, a needle and syringe or vacuum device and a band aid. We all have had blood drawn like this and it is no big deal except for those of us with aversions to needles. This simple test would answer the most important question. If the contact (which was later disclosed to be a household contact, which makes this even more likely to be related infections) is negative for antibodies, then great; we can let this go. But, if positive, then we need to explore the timing of onset of their respective symptoms and a detailed review of their activities and contacts during the days leading up to their infections to better understand did one infect the other or did they most likely have a common source exposure.
Another week later the CDC informs us that no source has been identified for the patient’s avian influenza infection (this means that this case is distinctly different than all the other known cases, and remains concerning for community spread because there has been adequate time for the epidemiological investigation to be completed). Now we are told that there were two health care workers who were exposed to the index case (the hospitalized patient) who subsequently developed respiratory symptoms after caring for the patient before respiratory precautions were put in place. One tested negative for influenza during the illness, serology testing was pending for the second case.
Then, we get a bombshell update on September 27 from the CDC. An additional four (i.e., now total of 6) health care workers developed respiratory symptoms following the identification of the index case (hospitalized patient), and 3 of the 4 (5 of the 6) were exposed to the index patient. However, unlike the initial two health care workers who were exposed prior to the institution of respiratory precautions (droplet), the subsequent three had exposures after those precautions were instituted. Drawing some inferences from the statement, it appears that serological tests (antibody testing) is pending for five of these health care workers (apparently, serology is not being performed on the first health care worker who is the only one who had PCR testing for influenza [that individual tested negative]). Frustratingly, the serology testing for the household contact of the index case is still pending.
We are also told that a total of 94 people were exposed to the patient while hospitalized.
So, why am I frustrated and why are so many experts troubled by this situation?
The fact that the CDC must be invited in to an outbreak investigation by the individual state is reminiscent of the frustration the world experienced as the WHO was unable to investigate the SARS-CoV-2 outbreak in China until it was invited in.
Similarly, the CDC and USDA have limited ability to surveil and manage the H5N1 outbreak on U.S. dairy cattle farms, which has resulted in undertesting, delays in identifying cases, a lack of ability to determine the full extent of the outbreak, and a failure of containing the outbreak.
The fact that we are still waiting on serological testing results from the household close contact of the index case at 3 weeks now indicates the bottleneck in testing (apparently this testing can only be done at the CDC lab reminiscent of the bottleneck in testing and marked delays in obtaining results that we experienced at the beginning of the COVID-19 pandemic, which blinded us to the extent of community spread of the disease at the time). It also suggests inefficiency of testing. I can generally get serology tests back in 48hours to a week. If there is a reason that this testing takes weeks to perform, then again, the CDC should just tell us. Otherwise, it feels as though they have the results and are not disclosing them, or they are slow-walking the testing.
The fact that it has taken so long to identify health care workers exposed to the index case and those who experienced symptoms suggests a lack of a sense of urgency in the investigation.
We are now told that the serological testing of the newly identified symptomatic health care workers will be delayed due to the weather conditions created by hurricane Helene. This is another problem with having only one laboratory (in Atlanta) that can perform this testing. I do not mean to imply that serologic testing is simple, however, it is done many times a day in thousands of laboratories across the country. If there is a reason that this testing can only be performed at the CDC in Atlanta, then just explain that to us. Otherwise, there are many laboratories across the country certified to conduct complex testing, and an effort should be made to speed up this testing and increase its availability now that we have a case that should be considered evidence of community spread, until proven otherwise. (We assume community spread when we cannot identify a source of the infection).
Recall, that at the time of this patient’s hospitalization August 22, we were at very high levels of COVID-19 across the country. In fact, it would not be surprising that some of these symptomatic health care workers had COVID and not bird flu. However, this is emblematic of the unexplainable, and I think, indefensible, abandonment of infection control practices in hospitals.
Let’s go a little deeper. So, we are told 94 health care workers were exposed to the patient. That means the patient was exposed to 94 health care workers when COVID levels were extremely high.
We are also told that initially no respiratory precautions were in place upon the patient’s admission. We aren’t told what the patient’s presenting signs and symptoms were (something that frustrates many of us that are trying to learn from these cases), but we are told that the avian influenza infection was picked up through the state’s seasonal flu surveillance system. So far, I have not been able to locate the exact criteria used for selection of patients to screen for influenza under Missouri’s surveillance system, but it would make sense that specimens would be obtained from patients with influenza-like illnesses (acute respiratory illnesses, fever, cough, etc.). It can certainly be difficult to distinguish influenza, COVID-19, RSV and a number of other respiratory infections early on in the course of hospitalization. Assuming this to be the case, and I fear that this hospital is no different from most across the country, patients with potentially contagious respiratory infections are being admitted without respiratory precautions, repeatedly exposing staff. And, of course, this also means that patients who already are vulnerable due to the illness they are hospitalized with are exposed to staff and to patients with respiratory infections for whom no respiratory precautions are in place.
Further, note of the 6 health care workers that so far were identified as developing respiratory symptoms after exposure to the patient, only one was tested while ill. That means that we don’t even know the extent that infections are being passed around in hospitals from patients to other patients or health care workers, or vice versa. We also aren’t provided with any information from the CDC’s update as to whether any of these symptomatic health care workers continued to work while they were symptomatically ill (spread to other patients or staff who were now contacts of the health care worker, but not the index patient?), and if they did, whether they were required to wear a respirator mask (I might fall out of my chair if the answer is yes).
It’s not like this is just all academic. If there is human-to-human transmission of this avian influenza, this is critical to know. It should inform farm and hospital infection control practices and how we handle infections. If there are sustained chains of transmission, then this is of paramount importance, because this means there is a pandemic threat and this calls for an active public health response and an updated pandemic response plan.
The CDC tells us that the public threat remains low. That is very possibly the case. However, that is an assessment based on very sparse and insufficient data. If the seven symptomatic close contacts are all negative on their serology testing, I would totally agree. If the seven symptomatic close contacts are all positive on their serology, then we have either got a highly infectious disease with an effective reproduction number of near 7 (the index case infected 7 people; for a pandemic to occur, one only needs this number to be greater than 1 if the other criteria we discussed above are met) or there is far greater community spread (i.e., not all of these people were infected by the index case, therefore there are many other undetected sources of infection out there) that we don’t know about. If it is the latter, and we simply have 6 out of 94 health care workers previously infected by someone other than the index patient (and we are not told that any of the remaining 88 health care workers are being tested in the event they had asymptomatic infections, or were pauci-symptomatic and their symptoms were so mild that when questioned weeks later they forgot about them), then we have already lost control of this.
For now, we will just wait for the drips of continued updates and try to piece this altogether as we get additional information that we should already have by now.
I do not recall a time that a college football game was cancelled due to a pertussis (whooping cough) outbreak, but that was just recently the case when an outbreak occurred among members of the Portland State football team just before they were scheduled to play South Dakota. That game was cancelled, and for a while, it was uncertain whether Portland State would have to cancel its scheduled match-up with Boise State, as well, but that game was able to go forward on September 21 – this past weekend.
Meanwhile, here in Idaho, the Bonner County Daily Bee Pertussis outbreak continues in region | Bonner County Daily Bee is reporting on a pertussis outbreak in the Panhandle – northern Idaho. According to reports from the Panhandle Health District as reported in the article, “Since April, the number of reported pertussis cases in North Idaho has grown from a few dozen to 166 as of mid-September, and that number is continuing to increase.” Keep in mind, the number of actual cases is almost certain to be far more than the number of cases reported, as not everyone with pertussis seeks or requires medical attention.
For comparison, Panhandle Health District only had nine total cases of pertussis over the past three years — five in 2023, three in 2022, and one in 2021.
The CDC also reports that cases of pertussis in the U.S. are on the rise this year. So far this year, cases are about three-times that reported in 2023.
One reason I was surprised about the outbreak among members of the Portland State football team, besides the fact that I had never heard of a college game being cancelled for this reason, is that although people of all ages can get pertussis, it is largely a disease that affects children and adolescents. Babies younger than one year old are at greatest risk of getting pertussis and developing severe complications. Of infants who develop whooping cough, roughly one-third need to be treated in the hospital. Whooping cough is particularly dangerous for these babies and infants because their airways are smaller and less well developed and generally, they have no prior existing immunity unless their mothers were vaccinated against pertussis during the pregnancy.
Pertussis is highly infectious. It is caused by bacteria called Bordetella pertussis. It is transmitted through respiratory droplets, predominantly, by coughing, sneezing, or even normal breathing when in close contact with others. This bacterium attaches to cells lining the upper airways that have hair-like extensions that act to help mobilize secretions and debris that we breath in from the air – these hair-like structures are called cilia (pronounced sil-E-ah). However, this bacterium releases a toxin when it infects cells and this toxin damages the cilia and often causes the airways to swell. This can cause choking, paroxysms of coughing sometimes severe enough and prolonged enough to cause vomiting, and in these young children, it can lead to a characteristic sign that gives the disease its name – whooping. Often, after one to two weeks of first presenting as a cold-like illness, the coughing phase begins and these infants may have a series of coughing fits followed by what seems like a prolonged effort to get a deep breath in that is accompanied by this “whoop” sound and the infant’s chest may cave in a bit. Even more worrisome is that some babies don’t develop these signs, but rather may have periods in which they stop breathing (apneic spells). While most of these children will recover, tragically, about 20 babies die per year from this infection.
While older children and adults don’t generally develop compromised breathing, the coughing can be quite bothersome and, in some cases, pneumonia can develop. Pertussis can be treated with antibiotics. Often times, a physician will make the diagnosis empirically, i.e., simply based upon typical signs and symptoms being present, especially when an increase in cases have been reported in the community. However, pertussis can be confused with other illnesses like RSV (respiratory syncytial virus), COVID-19, and influenza, so when in doubt, testing for this bacterium can be done with a PCR test from a nasal swab, like most persons experienced early on in the COVID-19 pandemic when testing for the SARS-CoV-2 virus. Given how contagious this infection is, the decision may be made to treat others in the family with antibiotics who are not yet showing signs or symptoms of the disease prophylactically when someone in the household is infected.
We begin DTaP vaccinations for babies at two months old and use this vaccine for children up to age 7. The “D” stands for diphtheria, another bacterial (Corynebacterium diphtheriae) infection that results from the toxin produced by this bacterium that can cause a grayish membrane to form in the back of the throat that can interfere with swallowing and breathing and cause an emergency. The “T” stands for tetanus toxoid, the stimulus for the immune system to protect the body from the life-threating toxin produced by the bacterium (Clostridium tetani) that causes the disease tetanus or more colloquially known as “lockjaw.” Finally, the “aP” stands for acellular pertussis, and this component of the vaccine consists of several protein antigens (antigens are recognized by the body as not part of the body and stimulate an immune reaction and the production of antibodies and the development of cellular immunity) from the bacterium and is referred to “acellular” to distinguish it from earlier vaccines that contained the entire cell of the bacterium. The acellular form of the vaccine is used in most developed countries because it results in far fewer side effects.
We then shift to the Tdap vaccine once children are around 11 or 12 years of age, and continue with this vaccine every ten years to boost the immune response, which does wane over time. The lower-case letters for “D” and “P” reflect that the dosage (amount of the vaccine component) has been reduced. This is also the formulation we often recommend for pregnant women during the 27th – 36th weeks of pregnancy in order for the mother to form antibodies that are then transferred to the infant and help protect that newborn until we can begin the baby’s vaccination series at 2 months of age. Many physicians will also recommend that the father and grandparents who are going to be in close contact with the baby get this vaccine to reduce the likelihood that they get infected and then pass the infection on to the vulnerable infant.
My role of trying to educate the public about this developing pandemic and the actual and potential risks that SARS-CoV-2 infection presented back in the first two years, when misinformation and disinformation were rampant, and when the evidence was still unfolding, and especially prior to the availability of vaccines, was greatly challenging.
On one hand, there was the loud voice of minimizers who likened COVID-19 to a cold or possibly even the flu and discouraged precautionary measures, and on the other hand, but not mutually exclusive, a group of physicians with more promotion on social media, cable networks, and even some of the mainstream media, who advocated for the unhealthy and elderly to stay home, but to have children and young adults return to all their normal activities, including those known to be high-risk for infection, to promote infection with the pronouncement that our country would then achieve herd immunity and COVID-19 would no longer present a significant threat to society. One well-known and nationally renowned physician even wrote an article for a major news outlet that predicted that we would achieve herd immunity as a country by April of 2021. I tried to warn the public that that prediction was not based upon any sound facts or science and was completely unreasonable. In fact, nearly 3 ½ years later, we still have not achieved “herd immunity.” I wrote at length about what herd immunity is, what factors are necessary to achieve herd immunity, and why herd immunity was not a reasonable expectation with the SARS-CoV-2 virus, at least for the foreseeable future in our book, Preparing for the Next Global Outbreak: A Guide to Planning from the Schoolhouse to the White House, https://www.press.jhu.edu/books/title/12896/preparing-next-global-outbreak.
Another challenge that was frustrating and challenging to deal with was the fact that the public’s and government’s focus and attention was on hospitals being overwhelmed and people dying from the disease. I tried repeatedly to raise the point that it often takes years after we first recognize a new virus to determine the long-term health consequences of infection, and sometimes these consequences can be serious and even disabling. I urged people to consider that we may learn of such health consequences from infection with SARS-CoV-2, so those who were being encouraged to take a cavalier approach to this virus because they were not in any of the identified high-risk groups, might still want to take reasonable steps to minimize the risks of infection, or at least guard against multiple reinfections, which would very likely increase any such long-term health risks. It is hard to know if my warnings made much of an impact.
Unfortunately, since then, we have learned that there are many potential long-term health risks, some that I had not even contemplated, and that these risks do, in fact, appear to increase with increasing number of infections.
In this blog post, I am only going to review two studies (more to come). The first is a study that would never be approved in the U.S. because the study took healthy individuals and exposed them (we call this a challenge study) to SARS-CoV-2 to study the effects of infection. Published by The Lancet, the investigators of this study, Changes in memory and cognition during the SARS-CoV-2 human challenge study – eClinicalMedicine (thelancet.com), took 34 healthy volunteers who had no history of COVID-19 and who were tested by serology (antibody testing) to ensure that they had no antibodies to the virus that would suggest prior asymptomatic or pauci-symptomatic infection of which the subjects were unaware, and inoculated them (introduced the virus directly into their nasal passage) with the wild type (original strain) of SARS-CoV-2. The investigators then conducted cognitive tests on the subjects (some who developed evidence of infection: measurable and sustained viral loads by PCR testing and some who did not become infected who then served as the comparison group) during their period of quarantine and at 30, 90, 180, 270, and 360 days following their artificially-induced infections in order to compare the results to their pre-infection, baseline cognitive testing. Of the eighteen subjects that developed laboratory evidence of infection, one was asymptomatic and all the others suffered only mild illness (i.e., not severe enough to require medical attention or intervention).
The infected subjects demonstrated statistically significant lower global composite cognitive scores than uninfected volunteers, and this difference occurred both during the acute infection, as well as through the follow-up period of 1 year. Memory and executive function tasks showed the largest between-group differences and this was despite the subjects generally having no awareness of the cognitive decline.
Although this was a small number of subjects tested, it was concerning that cognitive decline was detected in all cases, whether the infection was asymptomatic or mild. It remains an unanswered question as to how many of these subjects ever returned to their baseline level of cognitive functioning. While these subjects were not aware of their cognitive decline, it is not uncommon for people during and after COVID-19 to report “brain fog,” which generally refers to loss of memory, difficulty focusing, and difficulty maintaining attention for prolonged periods of time. Keep in mind that these subjects ranged in age between 18 and 30; these were not elderly individuals, but rather young adults in the prime of their lives. It also raises concern that with this impact on young adults, what is the impact on children with still developing brains?
The second study was a review article published in the New England Journal of Medicine in February of this year: Long Covid and Impaired Cognition — More Evidence and More Work to Do | New England Journal of Medicine (nejm.org). I have previously written about some of the neurologic and psychiatric sequelae of COVID-19, but this study looks further into a recent analysis of the U.S. Current Population Survey that showed that after the start of the Covid-19 pandemic, one million U.S. residents of working age reported having “‘serious difficulty’ remembering, concentrating, or making decisions” than at any time in the preceding 15 years. While in the previous paper, the investigators established cognitive decline with infection with the original strain of SARS-CoV-2 that occurred even with asymptomatic or mild infection and persisted at least a year, these authors point to the fact that cognitive decline has been reported with every variant since the original 2019 virus.
Concerningly, these researchers state:
As compared with uninfected participants (control), cognitive deficit — commensurate with a 3-point loss in IQ — was evident even in participants who had had mild Covid-19 with resolved symptoms. Participants with unresolved persistent symptoms had the equivalent of a 6-point loss in IQ, and those who had been admitted to the intensive care unit had the equivalent of a 9-point loss in IQ.
They go on to point out:
Memory, reasoning, and executive function (i.e., planning) tasks were the most sensitive indicators of impaired function, and scores on these tasks tended to correlate with brain fog. Vaccinations provided a small cognitive advantage. Reinfection contributed an additional loss in IQ of nearly 2 points, as compared with no reinfection.
It is hard to know the significance of these findings without longer follow-up and surveillance. But, these findings are concerning enough that I believe it prudent to try to protect our children is schools with better air handling, ventilation, and filtration. It is frustrating to me that minimizers, promoters of herd immunity, disinformation purveyors, and even our own public health messaging no doubt contributed to such a high population infection burden. I hope all of these changes in cognitive function reverse over time, but given that prior studies have shown that imaging can detect structural alterations to the brain, including loss of brain tissue, I am skeptical that all persons will experience recovery.
Starting tomorrow (Monday, September 23, 2024), all U.S. households can once again request 4 free at-home rapid antigen tests for COVID-19 on the website www.COVIDTests.gov.
Before throwing out tests you may have at home already, keep in mind that for many, the expiration dates have been extended beyond the date printed on the packaging. To see if your tests’ expiration dates have been extended, go to At-Home OTC COVID-19 Diagnostic Tests | FDA.
UPDATE (9/23/24)
I tried to submit my own order today, but apparently there is a delay. The government now states that you will be able to order them by the end of the month (1 week from today), but I cannot find anywhere where they specify the exact day.
One caution: Be sure you use COVIDTests.gov and not COVIDTests.com (the latter is an active website for a private company).
Though it can lead to confusion, I can’t think of a situation where having more options as to vaccines wasn’t a good thing.
For the COVID-19 vaccines, having the Novavax option was a good solution for those who have fears stoked by prominent antivaxxers who have spread all kinds of disinformation about the mRNA vaccines altering our DNA (this would flunk them out of the first year of medical school) or a completely made-up assertion, unfortunately perpetuated by a state public health official and amplified by this same group of disinformation purveyors, that the Pfizer vaccine contains DNA coding for the Simian Virus 40 protein (it doesn’t, and even if it did, the vaccine production process would destroy the DNA to the point that the protein wouldn’t be capable of coding for the production of the protein) and that this will now lead to the vaccine causing cancer (it hasn’t and won’t). But, it is understandable that some of the lay public has heard such disinformation and is hesitant to get the vaccines as a result. Therefore, Novavax, which is based on protein technology that has been used safely in the U.S. and around the world for decades, may be a good choice for these folks to put their minds to rest since no genetic material (RNA or DNA) is used in the process of making the vaccine, nor is any contained in the vaccine.
Novavax is also a welcome addition to our COVID-19 vaccine offerings for those who have had significant reactogenicity (side effects like sore arm, swelling or redness at the injection site, fever, headache, muscle aches, etc.) since Novavax has repeatedly been shown to have far less reactogenicity.
On the flu vaccine front, the FDA gave us great news two days ago when it approved a nasal spray influenza vaccine that has been and continues to be available through health care providers, but now can be purchased at the pharmacy with a prescription and taken home for self-administration. This is the first flu vaccine that has been approved for self-administration, which may improve the convenience and access to the vaccine. Also, there are not an insignificant number of people (and especially children) who are afraid of needles, so this vaccine may encourage them to get the influenza vaccine that they might otherwise not get.
This influenza vaccine is called FluMist. It was first approved in 2003 (in 2003, the lower end of the age limit was 5 years, but in 2007, the FDA lowered that to 2 years of age) and covers human seasonal influenza A and B viruses (not the avian influenza or bird flu that you may have seen in the news lately), and is approved for persons aged 2 – 49 (that may seem strange to you; more on that below).
One difference between the nasal vaccine and the “flu shots” is that the nasal vaccine contains an attenuated (weakened) form of live influenza virus. Because the virus is not “killed” or “inactivated,” it does produce a more vigorous immune response in the nasal passages, and as a result can cause low-grade fever in children (particularly under age 6) and in all recipients, the most common side effects are runny nose and nasal congestion. Adults who report side effects are more likely to report a sore throat.
We are told that for those who wish to self-administer the nasal vaccine (age 18 and over) or who wish to administer the vaccine to a person under the age of 18 in their household, you will go to the website of a third-party online pharmacy and fill out a screening and eligibility assessment. If eligibility is confirmed, the pharmacy will write the prescription and ship the vaccine to the address provided.
Who should not receive the nasal spray influenza vaccine?
Children under the age of 2 years;
Adults 50 years old and older;
Anyone with a history of severe allergic reactions to an ingredient of the vaccine or to a previous dose of any of the influenza vaccines;
Children ages 2 years – 17 years of age who are on aspirin or salicylate-containing medications (these children are at increased risk for Reye’s Syndrome with live virus);
Children ages 2 years – 4 years with a history of asthma or wheezing in the prior year.
Anyone who is immunocompromised (they should receive the flu shots with inactivated virus);
Anyone who resides with severely immunocompromised persons unless they can isolate themselves for a week following administration of the vaccine;
People who’s spleen has been removed (usually following trauma like a car accident) or who have a non-functioning spleen (for example, sickle cell disease);
Anyone who is pregnant (this is precautionary; the vaccine does not appear to be absorbed systemically and there has been no documented transmission or adverse effects to the fetus, but it is considered prudent to administer the inactivated influenza vaccine to pregnant women);
Anyone with a CSF (cerebral spinal fluid) leak connecting to their mouth, nose, ear, or other place within the skull (for example, as a result of surgery or trauma);
Persons with cochlear implants;
Anyone who has recently taken influenza antivirals (oseltamivir or zanamivir within 48 hours; peramivir within 5 days; or baloxavir within 17 days). This is because influenza antivirals can reduce the effectiveness of a live virus vaccine.
Further, if you are older than 5 years old with asthma; have underlying medical conditions; have an acute illness, especially another infection; or have a history of Guillain-Barre Syndrome, talk to your doctor before ordering the FluMist vaccine. There was an elevated risk for Guillain-Barre Syndrome with the 1976 swine flu vaccine, but no association has been noted with vaccines subsequent to 1976 (we have not used swine flu viruses for vaccines since 1976). Thus, the risk for this condition appears minimal, but we nevertheless would generally not administer this vaccine to anyone who has been experiencing or recovering from Guillain-Barre Syndrome within the prior 6 weeks.
The age cut-off of 49 years for FluMist will seem strange to some readers, as this is unusual. As far as I can tell, it is based upon one study that did not show effectiveness of the vaccine in those in the age group of 50 – 64 years. There are certainly methodological criticisms that can be made about this particular study, but nevertheless, absent another study demonstrating effectiveness in this age group, the age restriction is appropriate. Further, those who are ages 65 years and older should receive the high dose or recombinant influenza vaccines (FluMist only comes in one dosage formulation). Suitable vaccines for those 65 years and older include:
Finally, keep in mind that the immunity from all influenza vaccines wanes and therefore, even though it is currently being offered and promoted by some pharmacies, it is best to wait until we start seeing rising cases of influenza where you live before getting the vaccine so that it will give you the greatest protection for the entire flu season, which can certainly last as long as 6 months. If you follow me on X or on the Idaho Matters radio show, I will let you know when I think the ideal time is to get your vaccines as we watch the influenza activity here in Idaho and around the country.
We saw an unprecedented global outbreak of the monkeypox virus clade IIb in 2022 that was eventually contained to some degree with education and vaccination of those at highest risk for infection, which for the most part appeared to be men who have sex with multiple male partners.
Most recently, a new outbreak of monkeypox virus clade Ib is happening in African countries that have never had clade I infections, which appear to be transmitted both by close contact and through heterosexual sexual contact. Clade Ia has been known to have a case fatality rate of three to ten times that of Clade IIa infections, but there is little doubt that the lack of health care access and infrastructure in Africa contributes to a higher mortality rate than would be expected in more developed countries. Further, both Clade Ia and Ib infections appear to be far more frequently occurring in children who can suffer higher mortality rates.
The outbreak was declared a public health emergency for the African continent by the African CDC, and then shortly thereafter, was declared a Public Health Emergency of International Concern (PHEIC) by WHO. Almost immediately thereafter, a small number of cases of Clade Ib cases were detected in other countries where citizens had traveled to Africa.
At long last, vaccines are beginning to be delivered to Africa, however, the amounts are far less than that required to vaccinate a sufficient part of the population to ensure that we can bring the outbreak under control and prevent more cases from appearing in countries throughout the world.
One strategy used in combating the Clade IIb outbreak was to administer the vaccine intradermally (immediately under the skin) at 20 percent of the usual dose given subcutaneously (a short needle that goes beyond the skin but stops short of the muscle). This method would then allow a single dose of vaccine delivered in the typical subcutaneous fashion to be stretched out to five doses by using the intradermal route. If this strategy generates the same or better immune response, it would allow us to vaccinate many more of those in Africa giving us a better chance of containing the spread of Mpox, especially since the normal vaccination schedule calls for a second dose to be administered one month later.
A paper entitled: “Reactogenicity and immunogenicity against MPXV of the intradermal administration of Modified Vaccinia Ankara compared to the standard subcutaneous route” was published as a preprint just several days ago Reactogenicity and immunogenicity against MPXV of the intradermal administration of Modified Vaccinia Ankara compared to the standard subcutaneous route | medRxiv, and offers us important insights. This study compared the reactogenicity (local and systemic reactions from the vaccine administration) and immunogenicity (strength of the immune response generated by the vaccine) between these two doses and routes of administration when this vaccine strategy was used in 2022 in Rome.
It was discovered that the intradermal route actually generated slightly higher levels of IgG specific (to monkeypox) antibodies, as well as slightly higher neutralizing antibodies (recall that neutralizing antibodies are those that bind to the virus and interfere with the virus’ ability to infect and enter a cell. You may recall from my prior blog posts that the antibody response is part of our humoral immune response. It certainly appeared that the lower dose given intradermally stimulated an equally, or slightly better, humoral immune response.
However, we had little data as to the effect of these different doses and routes of administration on the cellular immune response. Antibodies cannot enter cells, so their effectiveness is primarily directed at preventing virus from infecting cells. However, once cells are infected, it is the cellular immune response that is primarily directed at killing infected cells, and thereby killing the virus that has infected the cells, and at clearing the virus from the body to eliminate persistence of infection.
The wonderful news from this study was that the cellular immune response was equally stimulated by either route of administration, even considering the reduced dose with the intradermal route.
Finally, not surprisingly, the intradermal route was more reactogenic, however, both routes of vaccine administration were well tolerated by vaccine recipients.
With these findings, I hope that the African CDC, WHO and other groups who are assisting with the vaccine roll-out in Africa will authorize and utilize the intradermal, dose-sparing method so that we can vaccinate a much larger number of people quickly, though of course this study was conducted on Clade IIb virus and we cannot be sure the same results would be attained with Clade Ib, but there is reason to be optimistic, even while those studies are done to confirm. The downside is that intradermal administration is technically more difficult, but generally, most people can be taught the proper technique and don’t require too much experience to become proficient at it.
As I have written about previously, H5N1 is an avian influenza virus (“bird flu” as it is colloquially referred to) that normally infects waterfowl, who in turn infect domestic poultry and sometimes wild birds through contamination of their food and habitats with droppings as these waterfowl fly over or temporarily land in these habitats. The H5N1 influenza virus (a type A influenza virus, but not one of the human seasonal influenza viruses) infects birds by binding to α 2, 3 – sialic acid residues on cell surfaces that are abundant in birds. Fortunately, prior to 2022, this virus transmitted inefficiently to other mammals and humans, likely due to the fact that most mammals, and certainly it is the case for humans, do not have α 2, 3 – sialic acid attached to a sugar on the cell surfaces in the upper airways, but rather the sialic acid conformation in human upper airways is of the α 2, 6 type. While there have been infections in humans, until this year, these have generally occurred in persons with extensive contact with sick and diseased birds, such as poultry farm workers or those who worked at the culling facilities during outbreaks on poultry farms. Unfortunately, when avian influenza of the H5N1 type has infected humans, the infection mortality rate (# deaths/# recognized infections) has been exceedingly high varying anywhere from 40 – 80 percent, and seemingly posing the greatest threat to young children.
In March of this year, it was recognized for the first time that H5N1 was causing outbreaks among dairy farms in the U.S. Studies revealed that the virus infected the utters of dairy cows and the milk from these cows had extremely high levels of virus in it. It was latter reported that cows’ utters have both α 2, 3 – sialic acid receptors and α 2, 6 – sialic acid receptors raising concern that the infected utters could serve as “mixing bowls” in which the potential exists for cows infected with H5N1 influenza virus (a new revelation) could be co-infected with seasonal human influenza viruses (a long-recognized potential and growing concern as we approach our influenza season given the continued spread of H5N1 virus among dairy cattle). Influenza viruses are known for their “reassortment” proclivity, in which any one of eight gene segments can be swapped from one virus to another. The resultant virus could then potentially have the virulence (potential to cause severe illness or death) of avian influenza coupled with the increased transmissibility of human influenza viruses, significantly raising the potential for a pandemic, as has happened in the past when avian influenza and human influenza viruses infected swine.
The outbreak of H5N1 among dairy cattle has been concerning not only because natural infection of cattle was unknown prior to this year, but also because it is the first time we are seeing convincing evidence of forward transmission among mammals, increasing the concern that the virus is evolving in a manner that might allow the same to happen in humans, a requisite for the virus to be of pandemic potential.
[A note to readers to help avoid confusion. First, although the H5N1 is an avian influenza virus, now that it is spreading among dairy cattle and there is evidence that transmission between cattle is occurring (as opposed to each cow being infected directly from a bird), the virus obtained from cattle (generally in the milk of the infected cow) is referred to by some as “bovine H5N1 influenza virus.” Secondly, since there are limitations to the studies we can conduct on humans relative to infectious diseases, it is common to identify animal models of infection that tend to have similarities to human infections or modes of transmission to facilitate our study of the infectious agent and/or disease it causes. Ferrets are commonly used as an animal model for influenza virus due to the similarities of our respiratory systems. Mice are commonly used to examine the ability of the infectious agent to transmit to the unborn offspring during pregnancy or to their offspring through lactation.]
Mice can become infected with bovine H5N1 virus through ingestion of the infected cow’s milk, and the virus quickly spreads throughout the mouse organs. When the mouse ingests a high dose of virus in the milk, virus can be detected in the nasal passages, lungs and brain of the mouse by day 6. The study showed that mice can also be infected by intranasal inoculation of virus.
The study also revealed that ferrets could be infected by intranasal inoculation of virus and that ferrets can become ill. Virus in the ill ferrets could be detected in respiratory and non-respiratory tissues, including the eyes, brain, colon, liver, spleen, kidney and/or heart.
The investigators showed that infected mice could transmit the bovine H5N1 influenza virus to their pups likely through the milk of the mother. However, it did not appear that the mice could transmit the virus to other adult mice (through respiratory droplets or aerosols).
The investigators tested the potential for infected ferrets to transmit the bovine H5N1 virus by respiratory droplets by infecting some with this influenza virus and others with an H1N1 virus, for which respiratory droplet transmission among ferrets has already been demonstrated, by placing uninfected ferrets in cages in proximity to cages with infected ferrets. The ferrets were tested with nasal swabs every other day. The infected ferrets developed positive tests with high viral titers (suggesting that they should be infectious to the uninfected ferrets if respiratory droplets are a mode of transmission). None of the ferrets exposed to ferrets infected with the bovine H5N1 showed any signs of infection, nor developed positive nasal swab tests. However, one of four exposed ferrets did have low-level antibodies to the H5 virus, which suggests that there is only inefficient transmission of the virus by respiratory droplets in ferrets.
Of concern, the investigators showed that, at least in the laboratory, the bovine H5N1 virus showed the ability to bind both α 2, 3 – sialic acid and α 2, 6 -sialic acids, raising the potential that the virus has already adapted in cows’ utters to be able to infect the upper airways of humans.
The authors of the Health Affairs article argue that this latter finding is concerning, but does not necessarily mean that this virus will spark a pandemic. However, they caution that this situation demands a more vigorous public health response to ensure that it doesn’t. The authors point out that the true assessment of the extent of the H5N1 outbreaks among poultry and dairy farms is severely hampered by the voluntary nature of testing of these farms and the relatively low level of engagement by farmers. Even more lacking is testing of farm workers, which is essential to identifying the extent of spillover transmission to humans and for serial genetic sequencing to detect whether the virus has picked up genetic mutations known to enhance mammalian spread.
I quote the following paragraph from the article that precisely mirrors my thoughts on our response thus far:
Any effective pre-pandemic strategy must be based on sound and timely data. Waiting for H5N1 to declare its presence among humans would be to waste precious time and risk converting preventative measures into futile exercises in rescue and recovery. The COVID-19 pandemic taught the danger of getting caught flat-footed, yet policy makers do not seem to have learned the lesson.
The authors make another suggestion with which I whole-heartedly agree and was a lesson that should have been learned from the COVID-19 pandemic. That is to set up multiple testing centers across the U.S. to screen for H5 influenza cases and to allow for more prompt sequencing and reporting of positive specimens. They also point out the need for rapid tests for providers, and ideally even for home use, especially by those workers and their families that are currently identified at highest risk of infection.
Adding my own personal thoughts is that this will be increasingly important as we enter into our seasonal flu season in which positive cases of influenza A will likely be assumed to be the seasonal human virus, missing potential cases of H5 infection.
The authors point out the need for rapid initiation of antiviral therapy, the need to avoid delayed antiviral treatment to reduce the risk of antiviral-resistance, and the need for more research and development into more effective antivirals that are effective against all strains of influenza.
The authors point out the very real limitation of our monitoring for infections and investigations of outbreaks among dairy farms in that farmers are reluctant to have virus detected due to the financial harm that could follow and farm workers are reluctant to seek medical attention for illness due to financial limitations, lack of health insurance, and fear of loss of their jobs if they are sick. An adequate public health response will have to address these concerns.
Finally, the authors rightly point out that our current influenza vaccine technology is too slow to allow for a prompt pandemic threat response. Further, given that the avian influenza H5N1 virus is highly pathogenic in poultry and results in a high mortality rate and the need to cull large numbers of poultry to contain outbreaks, it may not make as much sense to rely on an egg-based vaccine method. We must develop new vaccine strategies.
It is notable that as many as 30 percent of patients with COVID-19 present with neurological symptoms. For some time now, we have had evidence that the SARS-CoV-2 virus can infect the brain based upon the findings at autopsy in patients who died from COVID-19 that the viral genetic material could be found within cells of the brain and within the cerebral spinal fluid. It has been clear for some time now that we can see acute infection present with neurological impairments, or neurologic complications can occur weeks to months following seeming recovery from the infection, as well as part of the constellation of symptoms and conditions that occur in association with Long COVID.
There have been a number of mechanisms for SARS-CoV-2 infection of the brain proposed, including the virus entering the neurons of the olfactory nerve at the back of the nose and travelling up the nerve (retrograde neuronal spread) to the brain, spread to the brain during the brief period of time that the virus gets into the bloodstream (hematogenous spread), disruption of the blood brain barrier that normally makes it harder for infectious agents to get access to the brain by multiple mechanisms, including through cytokine storm that has been associated with severe cases of COVID-19 in children and adults, and neuronal fusion by which SARS-CoV-2 infection of one neuron may cause the neuron to abnormally fuse to another neuron allowing the virus to freely move between the fused neurons. SARS-CoV-2 has also been capable of causing neurological complications and conditions other than by direct infection of the brain cells by causing blockages in blood vessels that supply blood to or drain blood from the brain or by the formation of blood clots that travel in the blood stream to the brain, causing a lack of oxygenation (hypoxia) to a portion of the brain resulting in tissue injury or death of brain tissue and neurological deficits related to the particular brain function conducted by the affected part of the brain.
Depending upon the parts of the brain affected and the extent of the involvement, patients with COVID-19 may experience headache, loss of smell or altered smell, loss of taste or altered taste, a range of visual disturbances, sudden weakness or loss of movement of an extremity, confusion, altered mental status (level of cognition or alertness or both), seizures, abnormal movements, dizziness, imbalance, slurred speech or inability to speak, altered gait, tremors, slow movements, increased muscle tone, and impaired memory, persistent ringing in the ears, loss of hearing, among other neurological signs and symptoms.
These signs and symptoms can be manifestations of meningitis, encephalitis, encephalopathy, ischemic or hemorrhagic stroke, and Parkinson’s Disease among others. Further, it has been well established that those at risk of dementia or with early stages of dementia experience an acceleration and worsening of dementia following COVID-19. There has been mounting evidence that SAR-CoV-2 infection of the brain can result in dementia and pathological findings that very closely resemble Alzheimer’s Disease.
There is mounting evidence that those who develop loss of smell with their SARS-CoV-2 infection may be at increased risk of developing neurologic sequelae and neurodegenerative conditions following their COVID-19 illness. We don’t know how long following infection persons may remain at risk for neurological conditions; however, we are gaining mounting evidence that prior infection with certain viruses may cause neurological problems many years later in life, e.g., enterovirus and human herpes virus with amyotrophic lateral sclerosis (ALS), influenza virus with Parkinson’s disease, and Epstein-Barr virus with multiple sclerosis (MS). For a more extensive review of this topic, see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7838016/.
“Brain fog” remains one of the most frequent neurological complaints of Long COVID patients encompassing such things as diminished ability to concentrate and focus, confusion, short-term memory loss and/or decreased mental acuity, and cognitive impairments can often be detected on testing.
Patients with preexisting neurological conditions may be particularly at risk for neurological deterioration with SARS-CoV-2 infection, particularly those with Parkinson’s disease or those who are at risk for dementia or have early onset dementia.
Those persons who were hospitalized due to severe COVID-19 may be at particular risk for neurological sequelae. A study of such patients demonstrated that slightly more than half reported awareness of cognitive decline, while all patients tested had worse cognitive scores among all domains of cognitive testing following discharge from the hospital when compared to healthy controls adjusted for sociodemographic factors. In addition, roughly three-quarters of patients reported at least mild depression, a little more than half reported anxiety, and more than a fifth of all patients reported severe depression. Of great concern was the fact that depression, anxiety and fatigue were worse in this group of patients at 2 – 3 years following their illness than they were at either 6 months or 12 months in this patient population, including the occurrence of new symptoms among some patients. Just short of 27 percent of these patients reported an occupational change, most commonly attributed to their poor health, and most commonly and specifically based upon cognitive decline.
There are many potential complications and conditions that can follow SARS-CoV-2 infection. Many of these are distressing and life-altering. In this blog post, I discuss some of these complications and conditions that are neurological or psychiatric in nature. I will discuss other complications and conditions in subsequent blog posts. Given that we cannot predict with confidence who will and who will not develop these conditions, the public would be well-advised to consider the potential for these health consequences in addition to simply the risk for severe COVID-19 or death when considering risk mitigation strategies and COVID-19 immunizations.
The FDA has authorized two new COVID-19 vaccines (Pfizer and Moderna) and is expected to authorize a third (Novavax) in the coming weeks. It is anticipated that the Pfizer and Moderna vaccines may start showing up in some pharmacies as soon as this weekend, with much more availability during the course of next week.
What is different about these vaccines?
All three vaccines are monovalent vaccines, which means that they are based on the spike protein of just one variant. All three vaccines are based on different and more recently occurring variants than the variant that served as the basis for the 2023-2024 updated vaccines that were made available last September (XBB.1.5). The Novavax vaccine that is awaiting authorization is based upon JN.1 and the Pfizer and Moderna vaccines are both based on the KP.2 variant.
Are these new vaccines booster shots?
Technically, no. A booster is another dose of the same vaccine previously administered in order to boost the specific immune response generated by that prior dose of vaccine. In this case, because all three vaccines are new formulations based on more recent variants, they are technically priming doses and will result in new immune cells developing in response to the new variant’s spike protein. For those (see below) who are eligible for a second dose of this vaccine due to age or underlying medical conditions, that second dose next year will be a booster.
Having provided the technically correct answer, there are ways that this priming dose does act in some respects as a boosting dose. For example, let’s assume that you were infected early this year. That infection was very likely due to JN.1 as it was so fit that it basically outcompeted all the other circulating variants and became dominant. If you survived the infection and have a healthy immune system, then you developed an immune response to the JN.1 spike protein. If you were to get the Novavax updated vaccine next month when we expect it to be authorized, then this priming dose will significantly boost the immune response you generated from that prior infection.
The other way in which these priming vaccines will still act in a conceptual way as a “booster” is that there are many parts of the spike protein that serve as antigens (meaning that our immune systems recognize them as not us and something to form antibodies against), and some of those antigens will still be in the new spike protein formulation, and there are other parts of the spike protein that stimulate another part of our immune system that is particularly important in protecting us from severe disease and in clearing the virus from our system that gets boosted with each dose of vaccine we get.
Who can get the new COVID-19 vaccines?
The FDA has authorized the new 2024-2025 Pfizer and Moderna COVID-19 vaccines for those 6 months old and older. The CDC has recommended that everyone 6 months of age and older receive an updated COVID-19 vaccine.
When should you get the new vaccine?
The answer to this question depends in large part on your specific risks, so check with your doctor, but here are some considerations:
If you received a second dose of the 2023-2024 updated COVID-19 vaccine (likely due to your age or underlying medical conditions) within the last two months, the CDC’s guidance is to wait until a full two months after that shot to get the new updated vaccine.
If you have had COVID-19 within the past three months, the CDC guidance is to wait for a full three months after infection to get the new vaccine.
If you are over age 65 or have underlying medical conditions, and especially if you fit into both categories and/or are immunocompromised, and you have not had COVID or a COVID vaccine in the past year, your immune protection has likely significantly waned, and therefore, you should seriously consider getting the new vaccine ASAP, especially since we are experiencing high levels of community transmission.
If you have had or have Long COVID, your risks for returning symptoms or worsening of symptoms appears to be increased with another infection, and therefore, you should discuss with your doctor whether you should get the new vaccine now and a second dose in 4-6 months.
If you are pregnant, you are at risk for more severe disease than a woman your age who is not pregnant, and there are risks to your unborn child, so discuss the timing for getting the new vaccine with your obstetrician or whichever health care professional is managing your pregnancy care.
If you have upcoming travel plans, especially to a foreign country, and want to minimize the chances of illness and hospitalization away from home, consider timing your new vaccine dose at 10 – 14 days prior to your departure. The same advice would be relevant if you have an upcoming event, e.g., a wedding, where there will be a lot of guests, especially many travelling to the event, due to the increased risk of exposures.
If you have had significant reactions to the mRNA vaccines (Pfizer or Moderna) or your doctor has advised you not to take them due to a reaction, or if you merely are concerned about mRNA vaccines, you may wish to wait for the Novavax vaccine to become available, which as stated above, is expected in the upcoming weeks. Novavax is a protein subunit vaccine that has a long history of use in making various vaccines and contains no mRNA. It also is much less likely to cause the same degree of side effects (sore arm, swelling, fever, muscle aches) than the mRNA vaccines.
For everyone else, this is a tougher question to answer. Right now, levels of transmission are high throughout most of the U.S., however, it appears that we may have just reached the peak and may be headed down. If you are not at high-risk, have kept up with the recommended vaccines, and are able to employ non-pharmaceutical measures to minimize your exposures (for example, working from home, masking when out in public crowds, avoiding large indoor gatherings, etc.) until the levels of community spread decrease significantly, then you may very well want to wait until the next new variant begins to make a surge here in the U.S. (there is already a new variant that is circulating in Europe, but it doesn’t appear to be spreading significantly here in the U.S. yet) in order to try to line-up your highest immune response to the time of greatest risk of infection, especially because if you are in this group, you are unlikely to qualify for a booster dose in the first half of next year, then waiting for the next surge to begin could be a reasonable option.
Which vaccine should you get?
Unless you fall into category 3, 4, 5, 6, or 7, in which case you should not wait for Novavax and get either one of the mRNA vaccines depending upon the advice of your physician, this is a really difficult question to answer, and in fact, there is no correct answer. We do not have recent studies that test these vaccines in head-to-head comparisons.
There is suggestive, but not conclusive, data to support that mixing up the vaccines (such that if you have always received the Pfizer vaccine, to now get a Moderna vaccine, and vice versa) might result is a somewhat broadened antibody response, though the data is not so clear-cut as to make this a formal recommendation. Frankly, if you have tolerated one vaccine in the past, just go ahead and get that one again. On the other hand, if one of the mRNA vaccines caused significant side effects, try the other, or if you are not at high-risk as I described above, consider waiting for the new Novavax vaccine to come out.
The tricky part of the question is whether the mRNA vaccines (based on KP.2) or the Novavax vaccine (based on JN.1) will be most protective against the variants that will emerge over the course of the next year. That is because we don’t know how this virus will mutate and/or recombine in the near future. There is a case to be made for advocating for either option, and in fact, members of the vaccine committee that made its recommendations to the FDA and vaccine manufactures were not all in agreement on this. The arguments for the mRNA vaccines (KP.2) include the fact that KP.2 is more recent than JN.1 and the fact that this variant developed some new, more immune evasive mutations, and since that contributed to increased fitness, those mutations may be more likely to be reappearing in new future variants. However, the exception to that rule already happened in the subsequent variant that followed KP.2 – KP.3.
The other school of thought relates to the evolutionary biology of viruses, and particularly the SARS-CoV-2). If you think of the evolutionary tree much the way you might think of a family tree with which readers are likely more familiar, that tree has a trunk that begins with the oldest ancestor(s), and then has branches that grow off of it depending on the degree of relatedness. Unlike family trees, the evolutionary tree for viruses is not always linear, and this is especially true of SARS-CoV-2. Thus, while one branch seems to be progressing and growing with serial minor genetic mutations, all of a sudden, we see a new variant that is different enough that it is starting a new branch. Thus, this school of thought argues that using the trunk of the tree (in this case JN.1 from which all of the variants we have experienced since the beginning of this year are descendants) would likely result in a closer match to future variants than basing the vaccine on a variant that is from a branch (e.g., KP.2).
You’ll find vaccine experts that are proponents on both sides of the argument, and the fact is that we just don’t know. Time will tell, but two things do appear clear to us. One is that now into our fifth year of the pandemic, every dose of past vaccines has added protection against severe disease – hospitalization and death – no matter how well or poorly matched to the circulating variant at the time of infection. The other is that getting the vaccine reduces your risk of Long COVID by as much as 50 percent. Recall that every infection you get, increases your risk for Long COVID. So, don’t agonize over this decision. Any vaccine is better than no vaccine, and we have every reason to believe that any of these vaccines will reduce your risks for severe disease and Long COVID.