Let’s get a few matters out of the way before we dive in.
- I do not receive any financial benefit whatsoever whether you receive or refuse any vaccine currently on the market or in development. I do not own stock in any pharmaceutical companies, vaccine developers, or companies that are involved in producing, distributing or selling ingredients for vaccines that I know of. (I qualify with the statement “that I know of,” because I do invest in mutual funds that include large numbers of companies and these investments are managed and moved around by professional fund managers, so I couldn’t even tell you which companies they are investing in or whether they might buy or sell shares at any given time.)
- I am retired, so I am not administering vaccines to anyone and therefore, do not stand to gain financially from patients receiving vaccines or from treating patients who get ill as a consequence of not being vaccinated.
- I am not on the boards of any companies that have a financial interest in or receive a financial benefit from people receiving vaccines or from spreading vaccine disinformation.
- I do not receive any compensation or have any sponsorships for my blog, my social media, my media appearances, or my views on scientific, medical or public health issues.
- I do not receive payment for appearing on the weekly local Boise State Public Radio show Idaho Matters hosted by Gemma Gaudette, and the views I express on that show are strictly my own.
- I do not speak at political events, partisan-sponsored conferences, or on cable network shows or podcasts that have political or ideological leanings.
- I am not paid speaker’s fees for any talks on COVID-19, vaccines, or related issues.
- I am a life-long, conservative Republican who has never run for or held a political position, nor do I have any desire or ambition to do so.
- I am a Christian and raised my children in the Southern Baptist Church.
- Bottom line – everything I do with respect to my attempts to educate the public about health issues is to give back to the community the benefit of my education, training, years of medical practice, and many more years of experience and learning as I have served in leading a large teaching hospital and then a large health system, because I feel blessed to have had all the opportunities that I have had, the tremendous opportunity to help people in their time of need, the many lessons I have learned, and I refuse to let all of it go to waste now that I am retired. Further, as a practical matter, I don’t care whether you get vaccinated or not. Chances are, I don’t even know most of the people reading this. But, here is what I do care about:
- I think people should make informed decisions about their health care choices. That means we doctors provide you with the information – pros, cons, risks, benefits – about medical interventions and then, you the patient, or someone on your behalf if you are unable to make the decision, get to decide whether to accept or refuse the intervention. I respect it when patients make their decisions – those are decisions for them to make. What I deeply resent is doctors who manipulate patients into making a decision in favor or opposed to an intervention for their own best interests, not the patient’s. Most recently, I am appalled at the doctors who knowingly spread COVID-19 disinformation because they could not honestly answer the conflicts of interest questions above the way that I did, and yet they don’t disclose those conflicts. These doctors may be motivated by greed, political aspirations, commitments to ideology over science, notoriety, the funding to travel all over the U.S. and world to appear at conferences as a speaker, or other reasons or combinations of reasons, but it is abhorrent to the oaths we took as physicians, it is antithetical to the teachings of the Bible, and it is a terrible embarrassment to the profession.
- I think truth still matters. Without truth, and people to stand up to lies and disinformation loudly and clearly, we breed distrust. And, with distrust of science, medicine, public health, etc., people get hurt. As one of the current anti-vaxxers stated, the best way to disrupt public health is from within. This may be one of the few truths uttered by this disinformation purveyor. I never imagined that I would see the day when antivaxxers would be on public health boards, serve as state public health officials or even be proposed for political appointment to head or oversee our federal public health agencies. Most people do not understand the terrible threat this poses, and frankly, those threats will be in greatest part to our children and grandchildren and their successors, which is the most appalling thing about all of this, because we should protect those who cannot yet make decisions for themselves.
- I am old enough to have seen the amazing progress that modern science and medicine has made. I was in training when we were first seeing patients with HIV, but didn’t know what that was, and every patient, young adults for the most part, died, usually in a short amount of time. We now have patients living out long lives due to antiretroviral treatments, and, as of last year, we even have three patients cured of this disease and several in long-term remission. When I started practice, the majority of children died of acute leukemias; today, the majority of these children can be successfully treated and survive. We have more understanding of diseases, more treatment options, new technologies available to us, and research is coming up with more treatment options. I don’t want to go back, and I don’t want children to have to suffer from preventable illness. It is the children who suffer the greatest impacts of the antivaxx movement.
Okay, with that out of the way, let’s dive in.
I can’t possibly address all the lies and disinformation being spread out there, but let’s take some of the big ones, and then I may tackle some of the other ones in future blog posts. My objective is not going to be to give you a complete treatise, listing every reason and every scientific proof to show beyond a shadow of a doubt that every particular item of disinformation is completely false, but rather, show you the clearest and most convincing proofs that are easy to understand why the assertions made by those promoting disinformation are false. I would certainly hope that when I can convincingly prove that a number of the main points being spread are false, that would be enough for you to realize those persons spreading those lies should not be trusted with the other statements they are spreading.
- The COVID-19 vaccines are not vaccines.
This is a very common refrain from at least one doctor who promotes disinformation. When you hear this, you can be confident that the physician is purposefully trying to deceive you and manipulate you, because even antivaxxers don’t buy this argument, and certainly no reputable physician does. Any first-year medical student can tell you that a vaccine is a substance (usually a protein, a toxin, or a part or the whole of a pathogen [e.g., virus or bacterium] that is introduced by nasal spray, swallowing or injection, to stimulate a reaction from the immune system so as to prime the immune system to respond faster to a future exposure to that pathogen in order to prevent severe disease and death. Since the development of mRNA vaccines, the definition needed to be expanded to not require the direct introduction of the antigen (that substance that triggers an immune response), but to include the injection of mRNA that provides the code for cells to produce the protein (antigen) that will then in turn stimulate the immune response.
In other words, a vaccine, as opposed to antibiotics or other medications, trains the body’s immune system to be on the look-out for, respond faster, and attack a particular pathogen to minimize the harm if and when that person is exposed to that infectious pathogen. It is an advantage for the person to get a “sneak peek” to the future invader, to recognize it, and to be prepared in advance.
This is exactly what the currently authorized and approved COVID-19 vaccines in the U.S. do, although two of them utilize mRNA technology (Pfizer and Moderna) and one uses a long-used and traditional protein subunit technology (Novavax).
Those who try to promote the idea that COVID-19 vaccines are not vaccines often point to the fact that the vaccine does not always prevent infection, transmission of the infection to others and/or illness. However, this represents a lack of understanding of vaccines or intentional deceit, and would mean that the majority of vaccines (that they have acknowledged in the past are vaccines and in fact often have acknowledged that they and their families have received) are not vaccines.
Many vaccines – for example, the polio virus vaccines, RSV vaccines, rotavirus vaccines, influenza vaccines and COVID-19 vaccines – are intended to prevent people from getting seriously ill, ending up in the hospital or dying. They do not provide for “sterilizing immunity” – the prevention of infection and the onward transmission of infection to others, and frankly, most vaccines cannot achieve this much higher standard that disinformation purveyors want you to believe is characteristic, and in fact, a condition of being a vaccine.
Prevention of severe disease is a tremendous benefit of vaccines. It saves lives and it relieves the burdens on our health care infrastructure during times of high levels of community spread of that infection. However, if the vaccinated person does get infected, he or she will reproduce virus and can potentially spread the infection to others.
Sterilizing immunity generally requires the maintenance of high levels of neutralizing antibodies (these are antibodies that can attach to the virus to block its entry into cells) and these antibodies must be located in the tissues lining that part of the body in which the virus invades. This is difficult for any vaccine to achieve, and it is even more difficult when the virus is mutating, recombining or reassorting rapidly (these changes in the virus protein can cause conformational changes to the protein [change its shape or configuration] such that the antibody cannot bind as tightly or cannot attach at all), which occurred with the SARS-CoV-2 virus due to uncontrolled spread due to low levels of adoption of nonpharmaceutical measures and low vaccination rates (including lack of access to vaccines).
Bottom line: The COVID-19 vaccines are vaccines. Every study has shown an antibody response following vaccination in immunocompetent individuals. They use the spike protein of the SARS-CoV-2 virus (Novavax) or mRNA to instruct cells to produce spike protein (Pfizer and Moderna) in order to stimulate an immune response (development of antibodies, among other things) so that if the person is infected subsequently, the illness will be less severe and less likely to require hospitalization or result in death. That is a vaccine – you introduce a substance that induces an immune response that helps protect against severe disease.
- The vaccine is not safe.
The current vaccines are safe and we know this because we monitor for adverse effects and hundreds of millions of doses of vaccine have been administered in the U.S. (that number was 676 million doses as of a year and a half ago). Safe does not mean there are no side effects. Injection site soreness, redness and mild symptoms are common to almost all injections whether vaccines or medications. Safe does also not mean that there are no adverse effects in certain individuals, even serious ones. If you review the package inserts of every prescription medication you can see that some people will experience adverse effects even with medications that we consider to be very safe. There is no over-the-counter medication or supplement that has not caused adverse effects in some people who take them (aspirin and acetaminophen (Tylenol) have caused death under certain circumstances). Safe means that adverse effects are infrequent, generally mild or resolve completely, and for serious adverse effects they are rare, not higher than the background rates in the general population, or they occur infrequently enough that a reasonable person would weigh the risks of the vaccine against the risks of severe disease and still opt to have the vaccine. Unfortunately, any vaccine or medication can cause harms and some people will be harmed. It is terrible for someone to be harmed when given something to try to help them, and efforts are made to make vaccines and medications as safe as possible. Anytime a vaccine is given or a medication prescribed the doctor and patient must weigh the benefits against the harms. Oftentimes, as with the COVID-19 vaccines, the potential harms with the vaccine are far less common and less serious than those same harms caused by actual infection (e.g., the risk of myocarditis).
- Infections are good for us and help build healthy immune systems. Vaccines harm us.
Here is the truth in graphs:
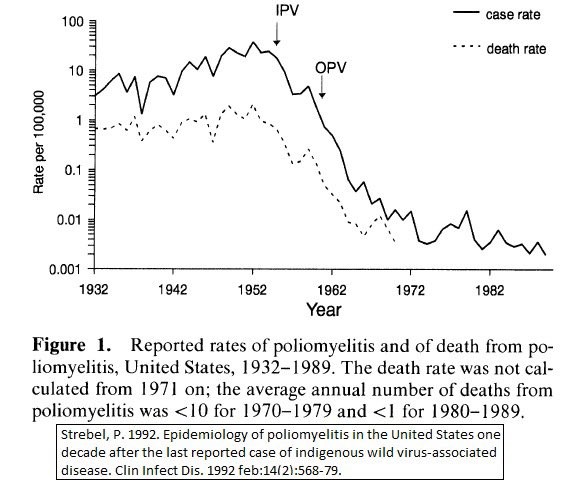
Poliomyelitis:
Note that the graph below has a logarithmic scale, not linear.
It shows the number of cases (solid line) of poliomyelitis (this number is far less than the number of infections, because few infections result in poliomyelitis paralytic disease and other manifestations of polio that are recognizable) expressed as the rate of disease in the population per 100,000 people, and this is only the numbers for the United States. It also shows the number of deaths also expressed as a rate per 100,000 people (dotted line). It is dramatic to see the decline in number of cases and in the death rate following the introduction of polio vaccines (first, the injectable vaccine – IPV, and then the oral vaccine – OPV, which those of us my age will remember as the “sugar cube”). It was because of these vaccines that we eliminated polio from the U.S.
Smallpox
Smallpox in its usual form (accounting for approximately 90% of cases) had a case fatality rate of around 30 percent. About 5 percent of cases were of the flat form (instead of the more classic fluid-filled blisters) that was fatal in 97 percent of cases. A hemorrhagic form accounted for about 3 percent of cases and was universally fatal.
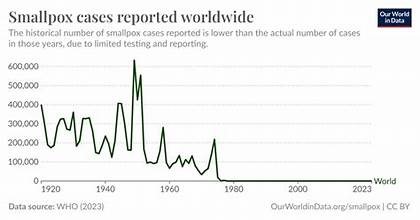
The smallpox vaccine was the earliest vaccine to be developed. In North America, through use of vaccination, smallpox was eliminated in 1952. It was finally eliminated in Africa in 1977, the last country in the world to achieve this goal and as a result, smallpox has now been eradicated across the globe, a remarkable achievement.
I could, of course, provide you with similar graphs of the reduction in number of cases and mortality rates due to vaccine-preventable diseases once those vaccines were developed and deployed, but for simplicity’s sake, here is some of that data in tabular form:
Effectiveness of Vaccination for some common Infectious Diseases in the U.S.
| Disease | Max. # Cases/Year | # Cases in 2019 |
| Diphtheria | 206,939 (1921) | 2 |
| Measles | 894,134 (1941) | 1,192 |
| Mumps | 152,209 (1968) | 3,780 |
| Pertussis (whooping cough) | 265,269 (1934) | 18,617 |
| Paralytic Polio | 21,269 (1952) | 0 |
| Rubella (German measles) | 57,686 (1969) | 6 |
| Tetanus | 1,560 (1923) | 26 |
| Hemophilus influenzae type B | Approx. 20,000 (1984) | 18 |
| Hepatitis B | 26,611 (1985) | 3,563 |
Source: Basic Immunology, Abbas, Lichtman, and Pillai, Elsevier 7th ed., Figure 1.2, page 3.
Vaccines have been one of the most successful public health interventions. In the pre-vaccine era, roughly half of all newborns died before their first birthday, largely from vaccine-preventable diseases. In the most recent data, that 50% mortality rate pre-vaccines in the first year of life is now 0.56%. Infant Deaths Have Risen for the First Time in 20 Years – The New York Times.
The truth is that our immune system is an intricate and very complicated system that serves to protect us from infection. Many infections can threaten our health and our lives. Vaccines are a way to prepare our immune systems to successfully fight off infections that might otherwise cause hospitalization and even death.
Vaccines can cause adverse effects in some people, however, at a population level, vaccines have saved hundreds of millions of lives.
- The COVID-19 vaccines were not effective.
The COVID-19 vaccines are in fact effective, and while I could provide mountains of evidence, I will just show you some data points that make this clear:
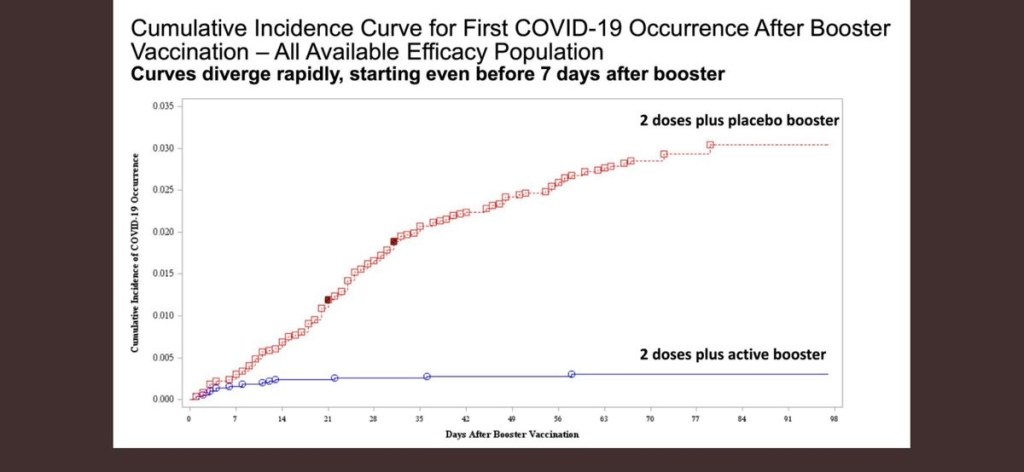
The above graph shows the effect of a COVID-19 booster in 2021 (this was the dose of vaccine given after the 2-dose priming series) on the cumulative incidence of COVID-19. Those who received the booster had a low number and relatively flat incidence of COVID-19, whereas those who did not receive the booster (received a placebo instead) had a steep increase in COVID-19 occurrences over the next three months.
As stated above, the primary purpose of the COVID-19 vaccines was to prevent severe disease. The vaccines were rolled out in 2021. Data from a six-month time period in 2021revealled that the average daily deaths per 100,000 people who tested positive for COVID-19 was 1.3 in unvaccinated individuals and only 0.1 in those who were vaccinated. Source: Basic Immunology, Abbas, Lichtman, and Pillai, Elsevier 7th ed., Figure 1.2, page 3. Further, throughout the time that the CDC reported hospitalizations and deaths from COVID-19 and compared those rates in patients who were unvaccinated versus those who were vaccinated, the rates in the unvaccinated were significantly higher.
The COVID-19 vaccines certainly can be improved upon, but it is clearly erroneous to state that they were not effective.
- The COVID-19 vaccines are causing “turbo” cancers.
This is a wild and baseless claim that asserts that the mRNA vaccines are causing a surge in fast-growing cancers, a claim that one particular disinformation doctor made soon after the vaccines became available (which in of itself made no scientific, medical or pathophysiological sense) indicating that he had seen a 20-fold increase in the number of cancers in his practice, even though he never produced the evidence for the claim and no laboratory anywhere in the world other than his had reported an increase in cancer diagnoses. There are many reasons that this assertion is nonsense, and only intended to promote fear of the vaccines, but here are some key reasons why this is ridiculous:
- The disinformation purveyors have made no effort to account for confounding variables. To understand confounding variables, let’s take an example. Suppose that I conduct a study that attempts to correlate student grades on the final exam in a college biology course with the number of hours the students spent studying for the exam. What I find is that those students who studied the greatest number of hours actually received lower grades than those students who studied fewer hours. I might very well make an incorrect conclusion that the longer one studies for a biology exam, the worse they will perform. Of course, that could be true, if for example, the students that performed worse, stayed up all night, were sleep-deprived and as a result, unable to concentrate and focus on the exam, whereas those who studied fewer hours were better rested. But, on the other hand, perhaps the reason that these students studied more hours is that they were cramming for the exam, whereas the other students had been studying all semester-long. Or, it could be that students who studied less had taken biology courses in high school and came into the course with a greater fund of knowledge. This is why we emphasize that correlation does not necessarily mean causation.
So, what confounding variables do the doctors touting “turbo cancers” disregard? First, let’s take a look at Differences in cancer rates among adults born between 1920 and 1990 in the USA: an analysis of population-based cancer registry data – The Lancet Public Health. The authors of this study examined the cancer incidence for 34 types of cancer and mortality trends for 25 types of cancer, by birth cohorts in the U.S. from age 25 to 84 for the period January 1, 2000 to December 31, 2019 (this is prior to the first identification of cases of COVID-19 in the U.S., and the vaccines wouldn’t be available to any Americans until a year later).
The authors found that the incident rates increased with each successive birth cohort for eight of the 34 cancers. These investigators found that there was an increasing incidence of 17 of 34 cancers in younger birth cohorts, adding to the growing evidence of increased cancer of increased cancer risk in younger generations. Thus, cancer risk was already increasing among younger Americans before COVID-19 and certainly before COVID-19 vaccines were made available to the public. Thus, any credible assertion that cancer rates are increasing or “turbo cancers” are developing requires that data account for this already increasing cancer risk. The problem is that those who spread the disinformation of turbo cancers offer no data. In fact, laughably, one such purveyor of this vaccine nonsense simply asks the room for a show of hands as to how many people know someone who was unexpectedly diagnosed with cancer, and then exclaims, “wow!” But, we don’t collect data by anecdotes or a show of hands. I suspect that most people reading this blog knew of someone who developed cancer even before the pandemic began since cancer is very common and is a leading cause of death.
Further, even if these doctors had data to show a significant increase in cancers after vaccines became available, there would also be the confounding factor that the vaccines were introduced because we had a novel virus infecting and sickening many more Americans than those that received the vaccine. Currently, there are seven viruses known to contribute to the development of cancer – Epstein-Barr Virus (EBV), Human Papillomavirus (HPV), Hepatitis B and C viruses (HBV and HCV), Human T-cell lymphotropic virus-1 (HTLV-1), Human Herpesvirus-8 (HHV-8), and Merkel Cell Polyomavirus (MCPyV). https://pmc.ncbi.nlm.nih.gov/articles/PMC5742800/. On the other hand, no vaccine has ever been demonstrated to contribute to the development of cancer. Thus, the burden rests with those trying to stoke fears about the COVID-19 vaccines to show evidence that it is the vaccines, rather than the SARS-CoV-2 contributing to the “turbo cancers” they assert are occurring, if in fact they have any evidence to support their claim of “turbo cancers.”
The attribution of any increase in cancers to vaccines has become even more difficult of a hurdle to meet because unlike the virus, for which there is accumulating evidence for possible persistence of virus, or at least viral proteins https://directorsblog.nih.gov/2024/10/31/many-people-with-long-covid-have-signs-of-persistent-sars-cov-2-proteins-new-findings-show/; all the evidence to date supports that the vaccine viral protein is cleared very promptly from the body. Thus, this presents even a greater challenge for those making the assertion of cancers due to the vaccines to explain why our long-standing concept that prolonged exposure (cigarette smoke, asbestos, and other carcinogens) is necessary for the development of cancer is wrong, and how a brief exposure to a substance could cause cancer and what animal model they can point to where that has ever been shown.
Without any data to support the notion of “turbo cancers,” without any accounting for the background rates of increasing cancer risk among younger Americans, without any explanation as to why if there was an unexpected increase it would be more likely due to the vaccines than to the infections themselves, without any explanation as to how a brief exposure to the spike protein in the vaccine would cause cancer but the much longer exposure to the virus proteins and in much greater amounts wouldn’t cause cancer, and with no experimental animal model to point to, these assertions can not be taken seriously and amount to complete fabrication by unethical doctors intent on stoking harmful and unjustified vaccine fears.
In closing, if you don’t want to get vaccinated, Godspeed. But, don’t let someone trick you and manipulate you into not protecting yourself and your family. Look at the facts and make an informed decision for yourself. But, if you don’t trust or want the COVID-19 vaccine, please don’t stop getting your children vaccines that have been used for decades, that we know are effective, and as you can clearly see for yourself have saved the lives of so many children.
Other Sources:
- Plotkin’s Vaccines, Plotkin, Orenstein, Offit, and Edwards. 7th edition. Elsevier. 2018
- Pollard, A.J., Bijker, E.M. A guide to vaccinology: from basic principles to new developments. Nat Rev Immunol 21, 83–100 (2021). https://doi.org/10.1038/s41577-020-00479-7.
- Explaining how vaccines work. https://www.cdc.gov/vaccines/basics/explaining-how-vaccines-work.html.


