For the past five years, we have been seeing the impacts of decades of coordinated anti-vaccine, and more generally and more recently, anti-science campaigns on a grand scale. When writing the previous sentence, I initially used the phrase “we have been seeing the end results,” but then I replaced “end results” with “impacts.” That is because, sadly and tragically, I think we are far from the end results that we will watch unfold over the upcoming months and years.
This is a difficult blog post for me to write because by nature, I am an eternal optimist, and that trait is aided and abetted by another trait in that I have a great propensity for being naïve. During the first couple of years of the COVID-19 pandemic, I optimistically and naively believed that (1) the pandemic would be our wake-up call to take infectious disease threats more seriously, and as a result invest more in research and preparedness (the exact opposite is occurring); (2) the clear and mounting evidence would persuade the citizenry and our elected leaders of the value of vaccines and the need to think about treating the circulating air in public buildings as a public health measure in much the way we thought about the need to treat water for public health back in the early 1900s (it didn’t); and (3) those doctors who promoted disinformation would be held accountable or at least fade away from the public light in shame (that largely did not happen).
As of April 17, 2025, the CDC has reported 800 confirmed cases of measles in the U.S. in 25 states: Alaska, Arkansas, California, Colorado, Florida, Georgia, Hawaii, Indiana, Kansas, Kentucky, Maryland, Michigan, Minnesota, New Jersey, New Mexico, New York City, New York State, Ohio, Oklahoma, Pennsylvania, Rhode Island, Tennessee, Texas, Vermont, and Washington. The number of actual cases is likely orders of magnitude higher as there are time delays in confirming and reporting cases, not all cases have sought medical care, and there have been reported to be some efforts among some communities to keep cases from being disclosed. Not only are the actual numbers almost certainly far higher, this outbreak is likely far from over. I will be surprised if this outbreak ends before the end of this calendar year and before extending to every state.
There are some interesting demographic data about these confirmed cases:
Under 5 years: 19% (47 of 249) 5-19 years: 7% (21 of 304) 20+ years: 6% (15 of 231)
Many people have the idea that measles would just be an issue for toddlers and preschoolers. But, as one can see, the outbreak is impacting children at all ages, including nursery, pre-school, elementary, middle school, high school, and even college. Some will be surprised by the number of cases in persons over 20 years of age. However, this is easily explained. The U.S. mounted a campaign to eliminate measles through immunization that resulted in measles cases precipitously dropping by 1991 and a certification that measles in the U.S. had been eliminated by 2000. Thus, persons born after 1990 (i.e., 35 years old and younger) who were not vaccinated, would have a fairly good chance of not having been exposed to measles and therefore susceptible to infection now. Further, I would suspect that a fair number of those that are over 20 years of age are also parents. If they were not vaccinated as children, there would be a good chance that they would not vaccinate their children and that many of these parents may have been infected by their children.
Another surprise to some may be that 15 of those over age 20 were hospitalized for measles. I actually am surprised that the number was not higher. Typically, those that are under 5 and those who are adults are the ones at highest risk for severe complications of measles such as pneumonia.
Further, as I have written before, this will not be the end of the health consequences from this outbreak of measles even once it does end. We know that those recovered will experience varying degrees of immune amnesia, meaning that they will lose some degree of their immune protection to other viruses as well as bacteria that they accumulated over the years, and as a consequence, their health risks and mortality rates are higher than the general population for the next few years until that immunity is reconstituted. Further, there is an absolutely dreadful and universally fatal neurological condition (subacute sclerosing panencephalitis) that, though fortunately rare, we are almost certain to see, probably in the next 3 – 7 years, due to the large number of people infected.
Much of what I wrote about above has been discussed with the public about the scale of this outbreak and the health consequences. However, what I have not heard is a discussion about is what other implications this outbreak has for us and our children and grandchildren.
While our focus has been on measles, it is important to realize that this same population of measles-susceptible individuals is also susceptible to rubella (German measles) and mumps since the vaccines for all three viral diseases has been included in a single vaccine – MMR – for their entire lifetime. Infection with measles provides no protection against rubella or mumps. It would not be surprising that measles would be among the first of these viral illnesses to emerge due to its high transmissibility and infectiousness, and the high levels of population immunity required to provide herd immunity (~95%).
I expect that we will see outbreaks of rubella and mumps in the months and years to come for a number of reasons. First, the wide-spread measles outbreak (over 800 reported cases as this time, however, I suspect that the actual number is in the thousands) is a good indicator of the number of children and young adults likely also susceptible to rubella and mumps. Measles is more highly contagious than rubella or mumps, and whereas the head immunity threshold is ~95% for measles (meaning that if a population has less than that number of its members protected against measles by virtue of vaccination or prior infection, then the potential for outbreaks increases significantly), that threshold for rubella is ~85% and for mumps is 85 – 90%. Thus, we expect measles to be the bellwether for disease outbreaks due to lack of herd immunity, but mumps and then rubella are certainly concerns to follow, unless high numbers of those not protected receive the MMR vaccine in response to efforts to contain the measles outbreak. Unfortunately, our federal response to the measles outbreak has not sufficiently focused on MMR vaccination, but rather confusing messages that tout various alternative approaches that we know do not prevent infection by the measles, German measles or mumps viruses.
So, let’s discuss these two other diseases and explain the concerns about their reemergence, if I am correct in my prediction.
Rubella (German measles)
As stated above, measles is the most contagious virus we know. Its reproduction number (R0), meaning the number of susceptible persons who are likely to be infected by one person with infection ranges between 12 – 18. German measles (rubella) is also transmitted by air and quite contagious, but much less so that measles. The R0 for rubella has been difficult to quantify and far ranging in various settings, but commonly believed to be < 5.
Rubella is caused by the rubella virus. Illness is characterized by fever, rash and swelling of the lymph nodes. Rubella is, in most people, a milder illness than measles, however, rubella has been a more common cause of birth defects than measles, and frequently, more severe defects. In fact, rubella has been the most frequent infectious disease cause of birth defects.
Rubella is a vaccine-preventable illness and the vaccine was approved in the U.S. in 1969. It was administered as a single dose vaccine until it was incorporated into the MMR vaccine in 1971 as a two-dose series. Through vaccination efforts, rubella was eliminated in the United States in 2004.
One of the feared conditions occurs when a pregnant mom is infected with the rubella virus, which can then pass to and infect the unborn child. That condition is referred to as congenital rubella syndrome. My fear is that many of the young girls and women who are infected in the current measles outbreak, will not seek vaccination against rubella, and that this will potentially give rise to an increase in congenital rubella syndrome in their future children.
Congenital rubella syndrome (“CRS”) is a constellation of possible manifestations that can include stillbirth, premature labor, brain structural abnormalities, liver involvement and enlargement, jaundice, growth retardation, cataracts, heart disease, and hearing loss. The risk of the fetus developing CRS is estimated to be 80% if the mother is infected with rubella during the first trimester, and this drops to a bit over 50% in the first part of the second trimester and then to 25% if the maternal infection occurs in the last part of the second trimester. CRS is a range of mild defects to severe, with severe occurring in roughly 10-20% of cases of CRS. The infants born to mothers infected in the third trimester can have congenital abnormalities, but they typically are milder and fewer and don’t present as the constellation of abnormalities characterized by CRS.
The last major rubella epidemic in the United States was from 1964 to 1965, and the toll was very significant. An estimated:
12.5 million people got rubella
11,000 pregnant women lost their babies
2,100 newborns died
20,000 babies were born with congenital rubella syndrome
In recent years, we typically have 10 or fewer cases of rubella infections per year and no cases of CRS. Most of these resulted from exposure during international travel or living abroad.
Mumps
The mumps virus is of similar contagiousness to the rubella virus with a R0 of just under 5 (about 4.8).
The mumps vaccine is very effective, however, unlike the measle vaccine which generally results in lifetime protection, the protection from the mumps vaccine does wane after 16 – 51 years, with an average of 27 years. So long as we continue to have high rates of vaccination such that 85 – 90% of the population is protected, older adults should remain at low risk even with waning immunity.
Mumps is generally a mild, though miserable, illness in children in which they experience fever and swelling of the parotid glands (these are salivary glands located over the cheeks just in front of the ears and extending down to the bottom of the jaw giving rise to a chipmunk appearance in children with infection), however, in rare cases, those infected can develop a serious inflammation of the brain requiring hospitalization that can cause death or permanent disability. However, as many as 10% of mumps infections acquired after puberty may cause severe complications including orchitis (swelling of the testicles), meningitis (inflammation of the lining around the brain), and deafness that can be transient or permanent. Orchitis can result in shrinking of the testicle or testicles and at least temporary loss of or decrease in fertility. Girls and women who are infected may develop oophoritis (an inflammation and swelling of the ovaries) and/or mastitis (an inflammation and swelling of the breasts).
In the case of measles and rubella, our concern in future outbreaks would be for those who are unvaccinated or those who are immunocompromised. However, if we do experience outbreaks of mumps in the future, we would be concerned that some young to middle-aged adults, as well as older individuals might be susceptible even though previously vaccinated due to waning immunity. If that happens, I suspect we would institute a third booster of mumps vaccine.
These would be truly sad developments given our previous success and knowledge accumulated over the years.
I have been writing about avian influenza since April 1st a year ago in a large number of blog posts.
To understand why I have written so much about this virus and why it remains a concern to me, let’s first review information I have previously provided and then let’s discuss an update and why there is growing concern.
Many of my long-term followers of the blog will recall that Dr. Epperly and I wrote a book entitled: Preparing for the Next Global Outbreak: Lessons from the Schoolhouse to the White House https://press.jhu.edu/books/title/12896/preparing-next-global-outbreak that was published by the Johns Hopkins University Press and released in April of 2023. In that book, we point out why we are at risk of future pandemics, why we need to prepare for them, and the lessons learned (117 of them, specifically) that should influence our preparedness and future responses to a pandemic. I also explained that pandemics are not 100-year events as commonly believed among the public, and why it would not be surprising for us to have another pandemic as soon as a decade from our last (recall that COVID-19 was declared a pandemic in March of 2020.)
Part of pandemic preparedness is surveillance of viruses with pandemic potential. (By the way, a pandemic does not have to be caused by a virus, and prior pandemics have been caused by bacteria, however, advances in science and medicine and the difference in transmission modes among viruses, bacteria, and fungi make viruses the strongest candidates for causing future pandemics.)
When I pick viruses for my list of those with the greatest pandemic potential, the criteria I use are:
1st level selection: Viruses with airborne transmission, i.e., the virus is emitted from the mouth and nose of the infected person in small enough particles that it can be carried large distances in an area with common ventilation (e.g., a home, classrooms, an airplane, public spaces) and can hang suspended in the air for some period of time. (examples are SARS-CoV-2, influenza viruses, and the measles virus).
2nd level selection: Of those viruses with airborne transmission, then I rank highest on the list those viruses that have the suspected or demonstrated ability for sustained human-to-human transmission and those that are novel viruses or known viruses with novel mutations, recombinations or reassortments for which there is expected to be little population-level immunity. (A novel virus is one that has not previously circulated in the current human population, and as a consequence, there is no or little existing immunity in humans and all or most all people would be considered susceptible to infection.)
(Levels 1 and 2 select for viruses with pandemic potential, then level 3 selects for the likely severity of the pandemic were it to materialize, which means not only would the virus be considered to have pandemic potential, but the pandemic would likely cause severe disease manifesting as the need for medical care and potentially hospitalization, be disruptive to society and its normal functioning, and have the potential for overwhelming our health care system.)
3rd level selection: Then, of those viruses that satisfy the first and second levels of selection, I rank those viruses with any of the following traits higher up the priority list, and even higher up the list based upon the number of these traits that they have:
Relatively high levels of morbidity (illness, but not death) and mortality (death) across all age groups, or at least many age groups;
Significant presymptomatic or asymptomatic spread of infectious virus;
School-aged children able to transmit the virus efficiently;
High infectious load of virus (the amount of virus in the nose and throat) in infected persons;
Low infectious dose required for transmission (the amount of virus that you must breathe in to become infected);
The virus is not particularly vulnerable to environmental factors (temperature, humidity, UV light) and is able to remain infectious in the air and on surfaces for an extended period of time;
No existing test or the only available tests are high complexity tests that can only be conducted in certain specialized laboratories (meaning that we will have trouble knowing the full extent of transmission of the virus in real time and we will not have the ability to quickly screen persons to determine whether they are infected with the virus);
Widespread zoonotic and reverse zoonotic spread (the virus can transmit among humans, to our pets and farm animals, and back to humans);
Non-durable immunity from infection and vaccination (meaning that reinfections will further increase the amount of disease transmission and illness, and the potential exists, as with COVID-19, that repeated infections will lead to long-term health conseequences);
No existing vaccine that is effective or that could quickly be modified to be effective in preventing severe disease;
No known existing medications with antiviral effect against the virus;
High degree of viral fitness and rapid evolution to increase transmissibility; and
Significant levels of infection among health care workers and nosocomial spread (this refers to patients infecting other patients and health care staff allowing for continued transmission chains among the most vulnerable people and the work force needed to care for patients) in health care facilities.
Using my criteria, avian influenza viruses and novel coronaviruses certainly have to be at the top of the list.
HPAI A(H5N1), an influenza A virus [HPAI is the abbreviation for “highly pathogenic avian influenza.” When referring to an avian influenza virus as being highly pathogenic we are indicating that it is a virus that causes death to all or the vast majority of birds (often chickens) that it infects as opposed to low pathogenic avian influenza viruses (LPAI) that do not typically cause severe illness or death in birds].
Let me take a moment and explain some of the nomenclature I am using. The A in “A(H5N1)” is an abbreviation for an influenza A virus (as opposed to influenza B, C or D viruses. A (other than the avian influenza viruses) and B viruses circulate across the globe in humans and generally cause seasonal epidemics annually. Influenza C generally causes very mild illness, and therefore, is not seen as a public health threat, nor is its activity tracked. Influenza D viruses circulate primarily in cattle, and we have not identified spillovers into humans.). The H5 refers to hemagglutinin subtype 5). The influenza virus has an envelope (not all viruses do), and hemagglutinin is the major protein found within the envelope. It is both involved as a site for binding to cells to cause infection, but also a target for neutralizing antibodies. There are 18 antigenically distinct (meaning that our immune responses to one form of hemagglutinin may provide little, if any, cross-reactive protection against another) subtypes of hemagglutinin protein – (H1 – H18).
The designation N1 refers to the fact that the other major protein of the virus is neuraminidase type 1. The neuraminidase is another envelope protein that plays a number of roles in the transmissibility of the virus, the infectivity of the virus and in the release of viral progeny once reproduced in an infected cell. There are 11 antigenically distinct subtypes of neuraminidase proteins – (N1 – N11).
A(H5N1) viruses are avian influenza viruses adapted to infect and transmit among birds because the cell receptor the virus attaches to that allows the virus to enter the cells of birds and replicate has an α-2,3 sialic acid sugar attached to the protein receptor whereas human influenza viruses utilize receptors on the cells of the human lung with α-2,6 sialic acid sugars that allows them to infect humans and transmit forward from humans.
The first identified outbreak of H5N1 was among poultry in Scotland in 1959. The first known transmission of this virus to a human was in 1997 in Hong Kong. In that year, a total of 18 persons were infected, and six of them died- i.e., a case fatality rate of 33%.
The predecessor virus to the one now spreading in North America has circulated in birds since at least 1996 (the first infection of the H5N1 virus that we are currently dealing with was detected in 1996 in China in a domestic goose) when it caused an epidemic among birds. The good news was that from 1997 until 2024, only a total of 902 sporadic human A(H5N1) cases had been reported from 23 countries, caused by different HPAI A(H5N1) virus clades.
Avian influenza viruses are of the N5 or N7 type. There are three avian influenza types that have been responsible for large disease outbreaks- H5N1, H5N8 and H7N9. Of these three, H5N1 is considered to be the most pathogenic and severe.
The first recognized transmission of the virus to non-human mammals was in 2021 to foxes. However, from late 2021 on, there have been concerning spread of the virus to an ever-expanding range of animal species and increasing numbers of infections within those species. Unfortunately, the wider geographic range of infections and the involvement of new species create opportunities for the emergence of new and potentially more dangerous variants of the virus. Further, the easy transmission observed between certain mammalian species, such as Spanish minks and Peruvian sea lions, raises concern about the potential for the virus to establish reservoirs in different animal populations and pose ongoing risks to both animal and human health.
Influenza A viruses are carried by wild birds in their intestinal tract and can be shed by these birds through various means, such as saliva, feces and nasal secretions. Transmission of HPAI H5N1 resulting in human infection primarily occurs through direct contact with infected birds.
The introduction of H5N1 into North America was not known to have occurred until late 2021, and this resulted from migratory birds. The bad news is that with ongoing transmission in animals, the virus does evolve and there is always the chance that it could mutate or reassort in a manner that would increase transmission to humans. In fact, the reference to different HPAI A(H5N1) virus clades is a reference to significant genetic changes to the virus warranting assignment to a new clade (for influenza viruses, we call these clades, but you can think of them as strains). The other bad news is that from 1997 to 2024, there is a cumulative case fatality rate of greater than 50% in humans.
In the last century, there have been four occasions when influenza viruses with genes that originated from swine (pig) or avian (bird) reservoirs entered the human population with wide-spread, efficient and sustained human-to-human transmission causing pandemics [1918 Spanish flu A(H1N1), 1957 Asian flu A(H2N2), 1968 Hong Kong flu A(H3N2), and 2009 swine flu A (H1N1)]. (Recall that I mentioned above that there is a common belief that pandemics are 100-year events, but obviously, this is not the case, and here I am only listing pandemics caused by influenza viruses.)
Thus far, while the H5N1 virus has infected humans, it has not shown the ability for efficient human-to-human transmission, and unless and until that happens, it will not produce a pandemic. Most of the infections have been in people with close contact with infected animals, and we have not seen much forward transmission, even to family members.
Then, why all the concern? The concern is that the virus is spreading globally, even to remote areas (including Antarctica), with an alarming expanded range of hosts, including occasional spillovers to humans, all of these events increasing the potential for mutations or reassortments that would all the virus to efficiently transmit to and among humans.
Waterfowl are natural hosts for low pathogenic influenza viruses. These wild and migratory birds then move to new locations and carry the virus with them. They congregate with domesticated ducks and geese to which they can transmit the viruses. Influenza viruses mutate frequently and while the virus started out as a low pathogenic virus (promoting its spread by these migratory birds that are not too sick to relocate geographically and find new domestic birds to transmit the virus to), there is the potential for the virus to evolve to a highly pathogenic form of virus that can result in loss of many domestic birds (some involved in our food chain) as it is transmitted among these birds and then potentially back again to migratory birds that can carry the virus to new areas of the state, country or world further infecting more domestic poultry before these birds die as appears to be happening with this current H5N1 epizootic.
What has been alarming during the past two years is that this particular HPAI A(H5N1) has been increasingly identified in mammals that generally have not been impacted by previous avian influenza viruses and we have seen the evidence that this particular virus can be highly pathogenic in many of these species of animals, as well, including ocean animals.
Human transmission of avian influenza viruses has historically been rare, as opposed to swine influenza viruses, which are much more suited for human transmission (while avian influenza viruses utilize only the α-2, 3 sialic acid receptors, swine have both α- 2, 3 and α- 2, 6 sialic acid receptors (the latter being the receptor type in the human lower airways), but still relatively uncommon (for example, we had three documented cases in 2023 (two in Michigan and one in Montana – all from direct exposure to pigs at fairs).
Swine flu is endemic to pigs. But pigs can be the intersection between birds (poultry on farms or even wild birds that transiently stop on land shared with pigs, or in the case of HPAI, where the bird carcasses remain following their death) and humans (farmers, visitors at fairs, live markets, etc.) and pigs can serve as a “mixing bowl” for human, swine and avian viruses when co-infected with both types of virus. “Mixing bowl” is a reference to the fact that coinfections of pigs with these different strains of influenza virus can result in the influenza viruses swapping segments of their genetic material, a process referred to as reassortment, in which the resulting virus has an increased ability to transmit from the pig to humans, and the most worrisome case being when the resulting reassorted virus also has the ability to transmit efficiently from humans to other humans. In fact, this is exactly what happened with the influenza A virus that caused the 2009 pandemic [A(H1N1)pdm09]. Genetic sequencing of this virus revealed that the eight gene segments of the virus were from a mix of avian, human and swine origins.
We have been experiencing an epizootic (an epidemic in animals) of avian influenza in dairy cattle in the U.S. for more than a year now, and we still have demonstrated little ability to contain the spread of this virus. The earliest detected cases were in Texas. This is also where we had the first detected spillover into a dairy worker.
We know where this virus came from: it’s a reassortment between Eurasian highly pathogenic avian influenza and low pathogenic North American avian influenza strains that were circulating naturally in wild birds.
While we have known for some time that cows could be infected with influenza D viruses, we previously had not observed avian influenza virus infections of cattle to any significant degree. And while we knew experimentally that virus could infect the mammary tissue of cows, mastitis was the common and prevailing manifestation of avian influenza infection in cattle, resulting in very high levels of virus in the milk of infected cows. An additional concern arose when it was reported by at least one laboratory that cow utters have both α- 2, 3 and α- 2, 6 sialic acid receptors giving rise to the theoretical risk that cows’ utters could serve as “mixing bowls” for different influenza viruses in addition to pigs.
Further, farmers started reporting deaths of domestic and peridomestic (wild animals that surround and come into frequent contact with domestic animals) on their farms, particularly grackles and pigeons and outdoor domestic cats who we believe contracted infection from drinking infected raw milk from the cows. Disturbingly, the cats known to be infected showed rapid and drastic neurological deterioration and death in the majority of cases.
We have now identified at least 70 human infections, with 1 reported death. However, more concerning are cases of bird flu of a different clade that are in migratory birds and have spilled over to humans. Most recently (April 8, 2025), a previously healthy, 3-year-old Mexican girl died from respiratory manifestations (respiratory failure) after a month’s long illness of avian influenza from a clade (D.1.1 transmitted by wild birds, compared to the B.1.1 and B.1.3 clades that have been transmitted by cows) of virus that is related to the case of a man in Louisiana who died from bird flu in January of this year (he was an older man and did have underlying medical conditions) from this clade of the virus. A person in Wyoming and a poultry worker in Ohio also were infected with this clade and experienced severe disease requiring hospitalization. A 13-year-old girl was also infected with this same clade and hospitalized in Canada with very severe disease requiring extraordinary care for a protracted period of time in the intensive care unit to save her life. Though these deaths are tragic, it might not be as concerning had these occurred in persons who had prolonged and close contact with cattle or poultry. However, most had no obvious source of contact with animals or exposure to account for their disease.
A case report in the New England Journal of Medicine provided us with important details about this first known transmission of H5N1 from a dairy cow to a human.
In late March of 2024, the farm worker developed redness and discomfort in his right eye. The worker denied having any fever, chills, cough, shortness of breath or loss or distortion of vision.
The worker denied any contact with dead or diseased birds or poultry. He did report close contact with cows, including cows that were showing signs of possible infection with avian influenza manifested by lethargy, fever, decreased appetite, dehydration, and/or decreased milk production. He did routinely wear gloves, but no other PPE including masks or eye protection.
On physical examination, the patient did not appear severely ill. His lungs were clear.
His eye examination revealed the following:
We are looking at the patient facing us, so the eye on the left side of this photo is actually his right eye, and the eye to our right is actually his left eye. Looking at his left eye, he has conjunctivitis (inflammation of the conjunctiva, which is the superficial lining of the eye and eye lids). We can see that it is red and injected, meaning that we see the blood vessels much more prominently than in someone with a normal-appearing eye. His right eye demonstrates a subconjunctival hemorrhage, in other words, there is bleeding directly under the conjunctiva. We can tell that there is a hemorrhage (bleeding) because the redness is confluent and obscures the blood vessels, whereas in his left eye, we can see the blood vessels much more clearly.
The examiner swabbed the patient’s nose and right eye to test for influenza virus. The test (which looks for genetic traces of virus) of both samples was positive for influenza A and for the H5 protein, which is indicative of avian influenza. That test also suggested that the amount of virus in the eye sample was very high. The CDC performed additional testing that confirmed that the virus was A(H5N1) and genetically the same as the virus detected to be circulating among dairy cows.
The patient was instructed to isolate at home and was started on an oral antiviral medication (oseltamivir). Over the ensuing days, the patient’s conjunctivitis resolved and no family members developed signs or symptoms of infection.
Additional testing of the virus genetic material revealed that it had not mutated in a way that would change the receptor-binding protein from the avian form (α- 2, 3-linked sialic acid [we do have this form or receptors in our eyes]) to the human form (α- 2, 6-linked sialic acid [this is the receptor type in the human respiratory tract]). On the other hand, the virus retrieved from the infected farm worker had acquired a mutation in the PB2 protein that has been associated with adaptation of the bird virus to mammals, including humans. Fortunately, the virus did not have the mutations that we associate with developing resistance to our usual influenza A virus antiviral agents.
This is good news/bad news. The bad news is that cows can transmit the virus to humans who are in close and prolonged contact with infected cows, though we still don’t know how transmission occurred – respiratory droplets from infected cows? Contact with virus in the milk of infected cows and then touching or rubbing one’s eyes? Aerosolization of virus from the milk when cleaning floors or equipment used in milking the cows?
The good news is that the patient did well and appeared to recover well, the virus did not show worrisome changes that would suggest that the virus can now efficiently transmit to and among humans, and the patient did not appear to infect anyone in his household, though we were not provided with any information as to what precautions were used in the home and how many persons were in the home. I suspect that the disease was relatively mild and mostly caused conjunctivitis is that the avian influenza virus involved had not acquired the ability to bind to α- 2, 6 sialic acid receptors and therefore, was unable to infect the person’s lungs.
There remain many questions. One question is whether the antiviral treatment prevented him from becoming more ill and/or did it shorten his course of illness? I also hope that they will carefully follow this farm worker over time. We know that in other mammals, this virus has seemed to produce significant neurological disease. The eyes can be a route for viruses to access the brain. It would be good to follow this patient to ensure he does not develop any signs of neurological disease in the future.
The continued transmission of A(H5N1) in cattle and in wild birds with spillovers to humans and domestic and peridomestic animals continues to concern me in that we are rolling the dice and giving this virus more chances to mutate and reassort. As I mentioned, this is an RNA virus and RNA viruses are more prone to acquire mutations because they often do not have the same proof-reading systems in place to catch errors when the RNA is being transcribed to produce viral proteins.
Many mutations are of no significance, some are detrimental to the virus and those viruses will generally lose in competition to more fit forms of the virus, so they disappear over time, and then some may be advantageous to the virus (increase viral fitness through increasing transmissibility, receptor binding or evading immune defenses).
The viruses that infected the cows and the humans that are generally causing conjunctivitis and mild illness are the same version of virus (B.1.1 or B.1.3). The viruses that have infected wild birds and then transmitted to humans causing much more severe disease are a different one that has infected cows (D.1.1).
We can look at the phylogenetic trees for this virus (you probably have seen these, but not known what they are called or what they mean, if you have followed the developments with SARS-CoV-2 over the past five years. These are diagrams that plot out the various versions of the virus starting (usually at the left side of the diagram) with the original form (wild-type) or at least the first discovered form of the virus and then those new versions of the virus with the fewest mutations will be closer and those with the most mutations will be further away from the original form of the virus. When the collection of mutations has been found to be significant, then the SARS-CoV-2 virus was assigned a new variant name (and appears on a new branch of the phylogenetic tree) or in the case of this A(H5N1) virus, it is assigned to a new clade.
We can look at a phylogenic tree for the changes in each of the viruses’ major proteins that we are interested in. We previously discussed the H or HA (hemagglutinin) protein and its role (especially in virus attachment to the host cell and fusion with the host cell’s membrane in order to allow the virus to enter the cell). This virus has the H5 subtype protein, and the phylogenic tree shows that there have been relatively minor mutations to this protein (that is good, because this protein is a vaccine target due to the fact that neutralizing antibodies are made to this protein as a result of infection). We can look at the tree for the N or NA (neuraminidase) protein (important in facilitating the release of newly formed viral progeny from the cell), in this case, the N1 protein, and see that it too, has relatively minor mutations, though certainly more than have occurred within the H protein (again, good news, because the H1 subtype is also a target for vaccines, but also of some of the antivirals we use).
There is a mutation required to the PB2 protein (not a vaccine target) that is necessary for transmission to mammals, though not sufficient in and of itself to allow for transmission to humans, and we see that has occurred, but only in the samples taken from infected humans, suggesting that this was an “in-host” mutation (occurred in the human after infection during translation and replication within human cells rather than in any of the cattle or prior bird samples). However, there are many more mutations to this protein and far more “divergence” (distance away from the prior forms – due to the large number of mutations), and I would not be surprised to find that it is developing in wild birds, and we are just not detecting it because we are not doing enough testing, as we did detect the mutation in a dead mammal. Perhaps one of these mutations explains the increased transmission in mammals.
Of course, this discussion just addresses mutations. As mentioned above, influenza viruses are known for reassortments with other influenza viruses, where they can exchange gene segments. This would potentially result in far more drastic change in the nature of the virus than simple mutations.
We fast forward to a year later and we now have concerning news coming from Texas dairy cattle. An article published in Nature Scientific Reports from March 14, 2025 titled “Superior replication, pathogenicity, and immune evasion of a Texas dairy cattle H5N1 virus compared to a historical avian isolate” reports on the development of a concern that I warned about last year. That is to say, if we allow certain viruses (especially RNA viruses, of which avian influenza is such a virus) to continue to spread, we risk the virus evolving and developing traits that can increase viral fitness, and potentially even develop changes that would allow it to evolve to infect humans.
The article reports that after spreading to nearly 900 dairy farms (including Idaho) and resulting in at least 39 (at the time of this study) known human infections, the avian influenza virus that has been spreading among cows has developed superior growth capability and rapid replication kinetics when studies in human lung cells in vitro (meaning in a laboratory setting as opposed to in the human body).
Worrisome for us, when the more recent isolates of the virus were tested in laboratory mice, the virus demonstrated more pathogenicity than earlier forms of the virus did, and infection in mice was accompanied by high virus titers in the brain and high mortality in the mice. Further, the virus had acquired new capabilities to thwart innate immune responses (these are our immune defenses that occur most immediately (as opposed to antibodies that take time to develop, don’t require prior exposure to the invading pathogen, and are far less specific and targeted than our antibody or cellular immune responses.)
A quick word on virologic studies. Information we gain from studies varies in its application to real-life human bodies and disease. For example, at the low end, during COVID-19 and future pandemics, we do studies referred to as in silico, which means that the study was done by computer modelling. For example, when we know the protein of a new virus that we want to target for antivirals or vaccines, the computer can generate a 3D model of the protein, as well as the medication of interest or the vaccine candidate to give us an idea as to whether the medication or vaccine might be likely to be effective. This is good for helping us prioritize our drug and vaccine candidates, but it only provides a low degree of confidence that the drug or vaccine will actually work in real life human bodies and in disease. For example, there were indications from in silico modeling that ivermectin might be a drug candidate because ivermectin appeared likely to bind an amino acid on the spike protein and an amino acid on the ACE-2 protein receptor. Further, it even seemed to be effective in the next step up of evidence, in vitro experiments, where we take a sample of the virus, a sample of human cells that the virus is known to infect and mix in the drug, in this case, ivermectin, in the laboratory to determine whether it impedes the virus from entering the cells, and it did. But, plenty of in silico and in vitro experiments that appear promising fail to pan out when taken to the next steps of clinical investigation.
When we have a promising drug or vaccine candidate, it is common to next move to studies in animals, particularly mice, because they are abundant, easy to manage, and cheap. The advantage of mice over laboratory experiments is that mice are living creatures, and unlike experiments in test tubes and cell cultures in a laboratory, they have circulatory systems, respiratory systems, immune systems, and actual functioning organs. This will often give us more indication as to whether the medication or vaccine that seemed to work in a test tube does work in a living being, however, mice still are much different than humans, and success in mice does not necessarily mean that it will work in humans leading to a common saying among scientists – “mice lie and monkeys exaggerate.”
However, different human diseases are often better suited to different animal models. For example, ferrets more closely resemble the anatomy and functioning of the human lung than mice do. On the other hand, mice develop cancers years faster than humans do, and so they can be very helpful in testing substances for carcinogenicity (the ability to induce cancer) such as has been done with food dyes. Again, mice are different than humans. When the substance does not cause cancer in the mice, that is reassuring, but not conclusive evidence that the same substance will not do so in humans, and conversely, if the substance does cause cancer in mice, that is concerning and calls for close observational studies in humans, but we often do not see cancer develop in humans.
When studies in common laboratory animals tend to further support the effectiveness of a drug or vaccine, it is common for us to then study it in larger animals that are more biologically related to us, especially mammals, and even better primates. These animals are much more expensive and it is harder to do studies in as large a group of these animals as it would be to do in mice. Studies in these animals are far more predictive of success or failure in humans and give us additional insights as to dosing and potential safety issues.
Now returning to the study referenced above, these findings related to increase in pathogenicity, severity of disease and antagonism of the innate immune response are important and concerning, but we have to keep in mind that they are results in mice, which may not be exactly the same in humans.
I’ll conclude with this. Whatever we think we know about this avian influenza outbreak in North America, particularly, the United States, it is an incomplete picture. Our government is not doing enough testing, surveillance and research into potential therapies and vaccines. The past administration did make an effort, but it was delayed and inadequate. Unfortunately, unconfirmed reports from people inside the CDC indicate that they are being told not to test dairy and poultry workers (recall the President’s comments in his first term when dealing with the COVID-19 pandemic – we wouldn’t have so many cases if we weren’t testing) and not to publicly report their symptoms. Many of the experts that were investigating and tracking this outbreak were fired in the government layoffs until someone realized this. Efforts were made to rehire them, but I don’t know how many were successfully retained. The NIH has made drastic cuts to research at a time when we need more influenza research. We are already suffering the loss of scientists from the government and universities due to personnel cuts and cuts to funding. Further, the Secretary of HHS is distracted and causing distraction by directing attention away from these real-time threats and to revisiting settled issues such as whether vaccines are associated with the development of autism, promoting elimination of fluoride from drinking water, and stoking the flames of a measles epidemic.
Again, I don’t know whether this will become a pandemic, but I can pretty much assure you that given all these changes, if it does, we will be delayed in recognizing it and we will be unprepared to deal with it. There is good reason to believe that this virus would be at least 20 times more fatal than SARS-CoV-2, and would kill many more children and possibly disproportionately so relative to older persons.
Long-time followers of my blog may remember the perplexing occurrence and significant number of cases of hepatitis (liver infection/inflammation) in 2022, first noted in the U.K. occurring in COVID-19-unvaccinated children under the age of 16 years that we have since referred to as acute hepatitis of unknown origin (AHUO) at a time when fewer mitigation measures were being taken to protect children in schools against airborne transmission of viruses. Clinically significant hepatitis is not a predominant feature of most cases of COVID-19, yet, many of these children were quite ill with the liver disease, some critically ill and still some requiring liver transplantation. Tests for the usual suspects (e.g., hepatitis A, B, C, D and E viruses) were all negative. After all the testing and review of cases, the major remaining differential diagnoses were narrowed down to adeno-associated virus co-infection with adenovirus or autoimmune hepatitis. We may now have a different answer.
We have known since the early days of the pandemic that SARS-Co-V-2 RNA can be detected in the stool of patients with acute COVID-19. Subsequent investigation and a publication by Zuo et al demonstrated that SARS-CoV-2 RNA can continue to be detected in some COVID-19 patients in the convalescent phase of the infection (when symptoms are resolving or have resolved).
Given mounting evidence of viral persistence in some people following SARS-CoV-2 infection and the fact that detection of viral RNA after the infection has supposedly resolved can be an indication of viral persistence, a group of investigators began to search for evidence of the virus in other organs of the gastrointestinal tract Residual SARS-CoV-2 viral antigens detected in GI and hepatic tissues from five recovered patients with COVID-19 | Gut. Using conventional immunohistochemistry (this is a process by which investigators create antibodies that are specific to the protein they wish to search for, tag these antibodies with a substance that will show up under the microscope, inject the antibodies into the tissues, then cut up the tissue into sections that can be stained and examined under a microscope), these investigators examined the tissues obtained from five patients who seemed to have recovered from COVID-19.
The protein they targeted was the nucleocapsid protein (NP) of the virus, as this protein is not present in any of the vaccines used in the U.S. or most other countries, only being an issue in the few countries that utilized whole inactivated virus in their vaccines, such as China. Thus, in those who have not received inactivated whole virus vaccine, the presence of NP (and by extension antibodies to NP) is a consequence and indicator of prior infection regardless of vaccine status.
These researchers detected SARS-CoV-2 NP in the colon, appendix (this is a finger-like projection extending from the colon very close to the location where the small intestine connects to the large intestine), ileum (this is the last part of the small intestine just before it connects to the large intestine (or colon), hemorrhoid tissue, liver, gallbladder and lymph nodes from these five patients who recovered from COVID-19, ranging from 9 to 180 days after testing negative for SARS-CoV-2 by nasal swabs. In fact, two of the five had NP detected in each of these locations, an indicator of how far and extensively the virus spreads within the body even in “mild” cases. The findings were validated by confirmatory identification of SARS-CoV-2 spike (S) protein and in some cases the presence of SARS-CoV-2 RNA.
Building on these two studies, with good evidence for viral persistence that can involve the liver as long as six months after even what appeared to be a “mild” infection, in an environment of a rapidly evolving virus with increasing immune escape capabilities, and especially at the time (2022) when we were seeing new Omicron variants as often as every several months, the case for autoimmune hepatitis has become strengthened.
Given the persistence of nucleocapsid protein embedded within liver cells following a prior infection, the potential for hepatitis due to cell-mediated killing of the liver cells as a consequence of efforts to clear the virus or autoimmune hepatitis upon subsequent reinfection with a similar, but distinct antigenic variant of SARS-CoV-2 are reasonable hypotheses.
These researchers examined the liver biopsies obtained from 12 patients (mean age 9.5 years) who were hospitalized between February 2022 and December 2022 in European countries who tested negative for acute adenoviral or SARS-CoV-2 infection and who met the WHO criteria for AHUO. Three of the 12 showed serological evidence of past adenoviral infection and 10 of the 12 had a history or serological evidence of past COVID-19. Eight of the 12 were known to have had a recent bout of COVID-19 with a median onset of 2 months prior to the hospitalization for AHUO. Unlike the original cohort noted in the U.K., a third of these children had a history of past COVID-19 vaccination.
Imaging mass cytometry (my apologies in advance to laboratory scientists who might be reading this as I have no expertise in this area – this is a technique that utilizes metal tags of antibodies designed for up to 40 antigens found in different types of cells that is applied to a tissue specimen. A machine then scans the tissue with a laser that generates signals from the metal tags that create detailed pictures of the cells in the tissue. The pictures reveal the location of the antigens targeted within the cells to allow identification of their intracellular locations as well as to help us understand how they are interacting with the cell) identified significant infiltration of the liver tissue with CD8+T- cells, which are cytotoxic T-cells (the cellular part of the immune response that identifies infected cells and kills them in order to rid the body of the virus within). The degree of infiltration and immune activation correlated with the severity of the hepatitis.
Further, the investigators detected SARS-CoV-2 antigens in ACE2- expressing cells in the areas of the liver with significant pathology in 11/12 samples using several different detection methods (we have known for some time that not everyone who has had COVID-19 will test positive on serological testing (measurement of antibodies in the blood).
The identification of immune-mediated liver injury associated with the detection of SARS-CoV- 2 antigens suggests a possible association of AHUO with prior SARS-CoV- 2 infection, further suggesting that the hepatic disease could have manifested as a part of Long COVID or post-acute sequelae of COVID-19.
PCR testing for adenovirus in liver specimens was negative in all of the subjects. Conversely, detection of SARS-CoV-2 proteins occurred in 11 of the 12 subjects. Notable was the extent of immune-cell infiltration in all subjects, and the degree of infiltration correlated with the clinical severity of each child’s course of illness. Further, the colocation of infiltrating cytotoxic T-cells in areas where SARS-CoV-2 proteins were detected suggests an antigen-mediated pathology.
The fact that the SARS-CoV-2 virus itself was not detected in the liver tissues and cells raises the concern that has already been raised as a possible underlying explanation for Long COVID, that virus is persisting and residing in areas of the body that are more difficult for the immune system to surveil and remove virus from (one candidate in these patients was already identified in the earlier studies I referenced above – the small and large intestines). In this instance, the thought would be that the persisting virus is replicating, although likely far less than in an acute infection, and shedding viral proteins that are entering the venous system that returns blood from the bowels that passes through the liver where the proteins can be deposited prior to the blood returning to the right side of the heart. Support for this theory is the fact that a biomarker for a disturbance of the gut integrity with subsequent leak into the vascular system (zonulin) has been detected in plasma along with spike protein. As a result, in at least some cases, immunopathology results and hepatitis may be the presenting illness as a result of liver cell injury due to the infiltration of immune cell infiltration targeting cells for destruction due to the presence of viral protein.
Of interest, this same situation of persistent SARS-CoV-2 virus in the GI tract with SARS-CoV-2 RNA detected in stool weeks after initial infection at a time when nasal swab testing for SARS-CoV-2 had long since turned negative has been postulated as the mechanism behind MIS-C (multi-system inflammatory syndrome in children) that we often saw present weeks to months following acute infection.
Of course, nothing from this study rules out the possibility that adeno-associated virus 2 (AAV2) contributes to the development or increases the risk for AHUO, but clearly, prior or co-infection with AAV2 does not appear to be necessary for the development of AHUO.
In conclusion, it appears that AHUO may be a post-COVID-19 immune-mediated hepatitis, another potential part of the spectrum of illnesses that may occur as part of the post-acute sequelae of COVID-19.
Kyle Pfannenstiel has excellent reporting in yesterday’s issue of the Idaho Capital Sun Idaho Legislature approves ivermectin deregulation, sending bill to governor • Idaho Capital Sun about the Idaho Legislature approving a measure to overrule federal law that requires ivermectin to be dispensed to humans pursuant to a prescription, which these Legislators believe will allow ivermectin to be sold over-the-counter in Idaho pharmacies and stores.
Here is the pertinent section of the bill that was just approved by the Idaho House and Senate:
“Notwithstanding any law to the contrary, ivermectin suitable for human use may be sold or purchased as an over-the-counter medication in this state without a prescription or consultation with a health care professional.”
The clause, “Notwithstanding any law to the contrary” might have been glossed over by those who don’t love legal jargon as much as I do or know what laws might be to the contrary, but there is an important law to the contrary – The Food, Drug, and Cosmetic Act that was enacted by the U.S. Congress.
The Durham-Humphrey Amendment divided drugs and medications into two categories: those that can only be sold and dispensed pursuant to a prescription and over the counter (OTC) medications that may be sold for self-administered use without the clinical oversight of a physician. The FDA has been delegated the authority to make the assignment of these two categories to those medications that can be legally sold in the U.S.
The Food, Drug, and Cosmetic Act has long been considered to be the supreme law of the land (that means overriding any state laws that are in conflict with the statute) and to displace states from this area of regulation that would otherwise lead to a patchwork of laws across the country. It has made sense to most of us that this would be the case as it allows for a concentration of expertise in a federal agency (the FDA) to undertake the lengthy and complicated issue of reviewing the basic science, animal and subsequent human studies of safety and efficacy for the myriad classes of medications to determine whether they are safe and effective, the appropriate indications for their use, the proper dosing and what side effects and adverse effects must be listed for health care professionals and for patients. I know of no states that would have this degree of expertise and infrastructure to both conduct the initial applications of medications and the post-marketing surveillance.
On the other hand, I did not fall out of my chair when I learned that the Idaho Legislature was considering this bill given what appears to me to be growing anti-science sentiment and a growing appetite to challenge federal laws by enacting state laws that are in conflict – a legal strategy that previously would have been sure to fail and considered a waste of taxpayer dollars, but more recently seems increasingly more plausible after EMTALA (the Emergency Medical Treatment and Active Labor Act) was found not to mean what its plain text says and what those of us who have studied it for almost 40 years always thought it meant.
Frankly, I fully expect one (or both) of two things to happen that will make the issue of Idaho law (assuming the governor does not veto the bill) in this instance being struck down a purely academic question and not one that sees the light of day in our hallowed halls of justice. First, I fully expect Dr. Martin Makary, the newly confirmed head of the FDA, who infamously pronounced that the U.S. would achieve herd immunity to SARS-CoV-2 and the pandemic would be over in just over one year (April of 2021), under the leadership of RFK, Jr., Secretary of HHS, will pronounce a recategorization of ivermectin to over-the-counter status. Second, even if I am wrong in my prediction, I cannot imagine a scenario where the current administration would attempt to enforce federal law and prevent Idaho from implementing this law. Without legal action by the federal government, there would be no case to be challenged in the courts.
Putting legal analysis to the side, there are so many disturbing issues about this latest action of the Idaho Legislature. These are not serious legislators and I will explain why below.
It would seem plain and obvious that if the legislature had never before entered into the field of regulating (rather deregulating) prescription medications and decided that this was now an area ripe for state regulation that it might want to hold some hearings, listen to some expert opinions, consider the implications of doing so (process, precedent-setting, legal, etc.), but that apparently didn’t happen. So, is the legislature going to embark on a review of all medications and make their own determinations as to whether they should be prescription or over-the-counter? If not, what will be the criteria for selecting which medications they will review? What criteria will they use? What expertise will they rely on? Personally, I have not felt that we need more government, more cost to taxpayers, and a legislature that needs to find more things with which to consume itself continuing its inching towards being a full-time job.
It would also seem plain and obvious that if the legislature is now going to undertake classifying medications, that it might want to hear from experts on the specific medications in question, let’s say maybe the board of pharmacy or maybe, in the case of ivermectin, some infectious disease experts? But as Mr. Pfannenstiel reported, “Idaho lawmakers didn’t hear public feedback on the bill from doctors, pharmacists or health care professionals.” That kind of makes me think that perhaps they merely want to pass something to score political points, but don’t want to be inconvenienced by hearing all the reasons that this might be a really bad idea or harm Idahoans. In fact, one only needed to listen in to the discussion to be aghast at all the misinformation and baseless claims made that would lead one to believe that ivermectin is nearly a cure-all, despite the very limited role for this medication in the evidence-based treatment of illness.
Of course, to the extent that the legislature is intending this to be their one and only foray into regulating medications, this is a problem of their own making. It was appalling to the medical community that the legislature actually promoted disinformation early on in the pandemic in giving unprecedented access to anti-vaccine messaging and late in the pandemic by introducing bills that would likely impair our response to future pandemics. (As an aside, the legislature is now recognizing the serious physician shortage such that it is contemplating the need to purchase a medical school while at the same time failing to have any insight that these anti-science/anti-medicine actions are undermining their stated objective of recruiting and retaining more physicians in Idaho).
It is a common strategy of antivax organizations to promote unproven preventatives and treatments to people to give them more confidence in refusing vaccination. Ivermectin was promoted on the flimsiest of data as a preventative against COVID-19 in the same way that vitamin A is now being touted as a preventative against measles. The problem is that well-designed, high-quality studies show that neither works. In the case of ivermectin, Idaho emergency room and critical care physicians often dealt with families who brought in a family member critically ill with COVID-19 only to learn that the assurances they received from a coordinated network of doctors touting their telehealth services for patients to receive ivermectin at a hefty cost were baseless. And, now Texas parents of children hospitalized for severe measles are learning that vitamin A not only did not prevent their unvaccinated child from getting measles, but that doctors are now having to address the harms the children have suffered as a result of vitamin A overdoses as well.
As Mr. Pfannenstiel points out in his article, “The U.S. Food and Drug and Administration, or FDA, hasn’t approved ivermectin to treat or prevent COVID-19, saying the federal agency finds existing clinical trial data don’t show “ivermectin is effective against COVID 19 in humans.” There are multiple high-quality studies that all support this conclusion, and I have previously provided and written about many of them on this blog.
The Legislature has pursued a number of bills that limit, restrict or even prohibit the use of a number of the tools that are available to address a future pandemic. There certainly are reasons to rethink a number of the approaches undertaken in the course of combating the COVID-19 pandemic. But, can anyone point to a committee or work group that has undertaken a review of our pandemic response and assimilated a list of lessons learned? Can anyone point to one bill that the legislature has introduced, held hearings on, and passed into law that would strengthen our pandemic preparedness? Please let me know if so, because I am not aware of anything as to either of these strategies that would seem to be the work of a serious legislature that wants to use real life lessons to help protect our state and its citizens.
How strong were the arguments of lay persons in favor of this bill? Let’s look at a couple:
According to Mr. Pfannenstiel, “Supporters argue making ivermectin more widely available for human use would avoid people buying versions of the drug intended for animals, and it would make human use safer by providing more information on appropriate doses.” This is illogical. First, the legislature didn’t buy analogous arguments for marijuana (and, by the way, I personally believe rightly so), so there is a problem of internal inconsistency. Second, the reason people were buying animal versions of ivermectin is because the state stood back and allowed certain physicians to promote disinformation that ivermectin would work and reputable physicians wouldn’t prescribe it because it was not safe and effective for the prevention or treatment of COVID-19.
Human use of a medication at appropriate doses does not make it safer if there is no benefit from taking the medication at any dose. Deceiving the public as to the benefits of ivermectin and then making it more available by making it over-the-counter does not protect Idahoans nor does it serve public health. In fact, given the implied claims of these disinformation doctors and appallingly some public health board members that ivermectin was essentially 100 percent effective in preventing SARS-CoV-2 infection and severe disease not only promoted the use of a medication that has potential adverse effects, while offering no benefit, but also gave many of these deceived Idahoans a sense of invincibility that actually increased their exposures and risks of infection mistakenly thinking that they couldn’t be infected while taking the medication.
In one example provided by Mr. Pfannenstiel, “Rep. Faye Thompson, R-McCall, said she recently went to a local feed store hoping to buy ivermectin for herself and her family to use, but stopped out of confusion over the appropriate dose.” This touches on the other issue that terrifies me about making ivermectin over-the-counter. I do believe that competent adults should be able to make foolish and irresponsible decisions if that is what they want and it won’t harm someone else. But, I fear that the fact that these same adults are already thinking that it is a brilliant idea to buy medications intended for animals for their children from a local feed store will mean they will give these over-the-counter medications to their children for inappropriate uses. Given that ivermectin is being already being touted by some of the disinformation doctors as a treatment for bird flu (a potentially lethal infection in children), a preventative and treatment for cancer, and God knows what all else, I fear that parents will resort to ivermectin rather than seeking medical care for a prompt diagnosis and effective treatment for potentially dangerous threats to the health of Idaho children. This would be a travesty.
Lest the reader of this blog post believe that this bill was just some fringe element of the Republican party, Mr. Pfannenstiel reported that this bill received bipartisan support, including only one vote against it in the House. One Democratic Representative that I had the impression was thoughtful offered his support of the bill on the basis that there are people who think ivermectin works comparing it to medical marijuana for the treatment of pain. I don’t know a single reputable physician or pharmacist that believes we should make all medications that people think works for something over-the-counter when the evidence clearly shows they are wrong.
I could go on much longer, but let me close with one horrifying thought. Mr. Pfannenstiel reported about one Idaho Senator giving credence to the notion that ivermectin is close to being a cure-all stating that “Some people will use it like taking vitamins.”
Measles is a highly contagious virus that causes infection (also called measles). Because it is so contagious, most people who have not yet been infected or vaccinated who are exposed to someone infected with the virus will develop measles.
How is measles transmitted?
Measles is spread by direct contact with respiratory droplets (spit/saliva/secretions emitted when someone who is infected talks, coughs or sneezes) and also by airborne routes (meaning that the virus can be suspended in the air and can expose people who are in the same room even if not close by or even by entering the room after the infected person has left until there has been enough air exchanges to remove all the virus).
What is the typical case of measles like?
Often a person who is infected will begin to feel very tired and easily fatigued, lose their appetite, begin to experience fever, will develop a runny nose and cough and pinkeye. Several days later, a red rash erupts, usually on the face, but gradually spreading down the body over the chest and abdomen, the arms and legs. The rash will often involve the palms of the hands and the soles of the feet. Patients often feel the worst during the first couple of days of the rash. In uncomplicated cases, patients tend to start to feel better and have resolution of the fever several days after the rash begins. The cough is usually the last symptom to resolve.
Why try to prevent cases of measles?
While many people recover uneventfully from measles, there are many alarming potential complications of measles and other than knowing that older individuals and those that are immunocompromised are more likely to develop severe disease and complications, we cannot predict which children will develop potentially life-threatening complications.
Prior to the availability of a vaccine, there would be as many as half a million cases of measles each year in the U.S. After vaccines were widely available, cases of measles in the U.S. were as low as 100 in a year. In the early 1960s, prior to the availability of the measles vaccine, roughly 8 million children world-wide would die of measles complications every year.
What are the complications that can occur after measles infection?
One of the most common and also unique complications of measles infection is what is referred to as “immune amnesia,” meaning that there is a loss of some of the immune protection the person had already built up prior to getting infected with measles either due to vaccination or due to prior infection. Researchers had noted that in the few years following measles infection, children seemed to have higher rates of infection and even more severe outcomes. When looking into why, they discovered that the measles virus is able to use a receptor on certain immune cells of the body to infect the very cells that produce antibodies and are meant to protect us from infection. Following measles, the researchers found that persons could lose anywhere from 11 to 73 percent of their preexisting antibodies to both viral and bacterial infections and that this loss of immune protection could last as long as three years. If you want more details, see https://www.science.org/doi/10.1126/science.aay6485.
The most common acute complications involve the lungs and the brain. Pneumonia accounts for about 60 percent of the deaths in infants with measles. Pneumonia can be caused directly by the measles virus or can be a result of a superimposed bacterial infection due to the damage caused by the measles virus that can facilitate bacteria invading the damaged lungs.
The brain complications most often manifest as a condition referred to as encephalitis (meaning an inflammation of the brain), and can take one of two forms. Acute (meaning occurring during the measles illness rather than after it) encephalitis is often recognized by a recurrence of the fever or fever that doesn’t resolve in the normal timeframe, along with headaches, seizures, and a change to the level of consciousness (less alert, confused, etc.). While most people survive this complication, prior to vaccines, some individuals would be left with deafness, blindness or other permanent brain dysfunction.
An even more dreaded, but fortunately rare, complication of measles is subacute sclerosing panencephalitis (SSPE), the other form of encephalitis, but unlike the acute encephalitis above, this encephalitis does not have its onset until years after the person has seemed to have fully recovered and it is uniformly fatal. Typically, others will note personality changes, the patient’s handwriting begins to clearly deteriorate, and they become forgetful. As the condition progresses, the patient becomes progressively less able to walk, stand, and even talk. The patient may become combative, begin to have seizures and eventually lapses into a coma.
Is the measles vaccine safe and effective?
Getting the measles vaccine to prevent measles infection is generally safer than getting the measles infection itself. The measles vaccine is highly effective and like the infection itself, confers life-long protection for most people. However, one of the ways this is achieved is by using the actual measles virus but pre-treating it so that it is in a weakened (attenuated) form. For healthy children and adults, the vaccine will not cause the measles disease and therefore will prevent the various complications from occurring. However, because the virus is not killed, the vaccine is generally not advised for people whose immune systems are weakened or otherwise compromised.
The vaccine is highly effective. A single dose is 93 percent effective on average at preventing measles and a second dose increases effectiveness to 97 percent on average.
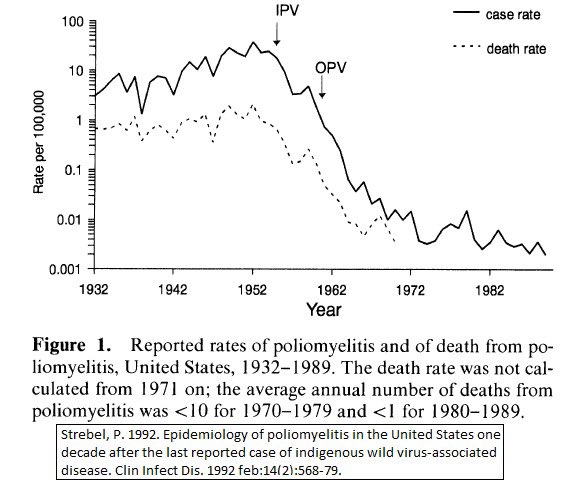
The following graph depicts the cases of measles in the U.S. before and after the measles vaccine was made available (1963):
In my prior blog post on Why Get Vaccinated and How Do Vaccines Work, I tried to explain what vaccines are, how they work at a very basic level, and the benefits of vaccines that might weigh in favor of immunization for those who have no or only a rudimentary understanding of vaccines, immunology and pathophysiology. I used analogies to try to give the reader a clear and better understanding of these concepts at a very superficial level.
In this blog post, I once again am going to use analogies in order to give the reader a possible conceptual framework for being able to weigh the risks of getting vaccinated versus getting natural infection in the context of a novel virus, like SARS-CoV-2. And, like in the prior post, we will go back to 2021 – a year into the pandemic with this novel virus and the time at which vaccines were being rolled out. I want to point out that this risk-benefit analysis that we are going to go through would be quite different than the one for a routine childhood vaccination that has been in use for decades or the risk-benefit decision for hopefully rare situations such as a rabies exposure or even the risk-benefit decision for a vaccine against a potential, but unlikely future infection (e.g., certain vaccines for international travel), and I am not going to address these situations in this post.
For this analogy, we will again go back to the beginning of 2021. The COVID vaccines were just being rolled out. We knew that SARS-CoV-2 was quite contagious and that it could be transmitted by people who were asymptomatic or had mild symptoms that they may have attributed to allergies or other noninfectious causes, and therefore, those persons might be at school, at work or guests in your home without knowing that they were infected and contagious. We also knew that older individuals, obese individuals, immunocompromised individuals and those with certain underlying chronic medical problems seemed to be at greatest risk for severe disease (low oxygen levels, the need for hospitalization, the need for critical care, or death). We were starting to observe mutations that appeared to enhance the transmissibility of the virus.
One of the most disappointing things to me was that we were also seeing a growing number of reports of reinfection, meaning that we could not count on an infection conferring long-term, durable protection from reinfection. At that time, we did not know the consequences of repeated infection, however, we had begun clinical studies to try to understand why some patients who survived COVID-19 had lingering illness (Long COVID) that in some cases was quite disabling to the patients, and in many cases delayed a return to work, prevented a full-time return to work, or in some cases patients were no longer able to perform their job duties.
The clinical trials of the two mRNA vaccines that were the first to be available in the U.S. had included 43,548 participants in the Pfizer vaccine trial (21,720 received the investigational vaccine, 21,728 received a placebo and served as the control group) and 30,420 participants in the Moderna vaccine trial (15,210 in each group). A serious adverse event occurring once in every 100 people would be a rate of 1 percent. So, both trials were designed to detect any common serious adverse events. If a serious adverse event occurred at a rate of 1 in every one hundred thousand or 1 in every million people, obviously, those might not show up until the vaccine was rolled out to the general public.
So, now let’s go back to early 2021. Vaccines are being rolled out. Vaccination of health care professionals and first responders had already begun. The elderly now would be able to sign up to get vaccinated and then the roll-out would continue to other groups. If you were a 30-, 40- or 50-year-old, married adult with kids and a spouse, in reasonably good health, but lets say a bit overweight and perhaps some mild hypertension controlled on medication, how might you think about whether to get vaccinated.
Let’s say that I told you at that time that during the next twelve months, there was a 75 percent chance that you would be involved in an automobile accident. What I can’t tell you is whether it will be a fender-bender; someone will just back into your car or vice versa; you will veer off the road and collide into a tree or your car end up in the river; your car will roll-over or be totaled and if so, whether you will escape unscathed, be killed or survive, but have multiple broken bones, a concussion or perhaps even lose a limb or be paralyzed; or whether it will be an auto-pedestrian accident in which you might be the driver or the pedestrian. I also cannot tell you whether you will be alone or have someone else in your car who will be harmed or not. I also cannot tell you whether you will be the driver or the passenger in the car.
[I picked the 75 percent number because in our analogy, the automobile accident is the analogy for getting COVID-19. At that time, we did not know what a person’s chances were of getting infected in the upcoming year, however, we know that by the end of that year based on antibody testing, roughly 75 percent of children and adolescents had been infected at some point during the pandemic, and possibly more than once. This is a good group to use for this analogy, because this is the group for which there were the fewest mitigations undertaken, and so, it is not unreasonable for us to use this as our baseline risk with no mitigations (working from home, avoiding large gatherings, physical distancing, having good ventilation, masking, etc.) for the adults in our analogy, especially because school-aged children are often the ones who are the index case (first infected) for spread of infection in a household. Now, in fairness, Dr. Marty Makary, the current nominee to lead serve as the FDA Commissioner for President-elect Trump wrote a Wall Street Journal op-ed published in February 2021 that we would achieve “herd immunity” by April, a prediction that some people may have in part relied on to decide against getting vaccinated early in 2021. However, as I mentioned above, in observing the increasing number of reinfections, I was telling people and writing in my book that herd immunity was very unlikely because we are not seeing durable individual immunity – a prerequisite for herd immunity. For purposes of this analogy, I am not going to factor that some people were likely duped by Dr. Makary’s article in believing that vaccination would be unnecessary because (1) it was obviously proved to be wrong even relatively early in 2021, (2) by that time, we were already seeing clear evidence of new variants emerging (alpha and beta by this point in time) that demonstrated that the virus was evolving and actually becoming more transmissible and likely immune-evasive, and (3) as I mentioned, we were still not seeing evidence of long-lasting, durable immunity from infection, without which herd immunity is not possible other than potentially with vaccines.]
So, if I told you about your 75 percent chance of being involved in an automobile accident in the coming year, what might you do differently? A lot of the answer depends on your “risk tolerance.” We all take risks every day. People have different tolerance levels for risk at different points in their lives and in part, based upon their life experiences (e.g., many who have never done so might fear sky diving and think about all kinds of risks that might come to fruition, where as someone with much experience and confidence might assess the risks as being much lower and very willing to do so. Even fewer might be willing to go base jumping (jumping off buildings, cliffs, or bridges with a parachute) and, I imagine that even many who might assess the risks of sky diving to be minimal, might be unwilling to accept the increased risks of base jumping, and, having run a health system that served an area that attracted base jumpers to a bridge over a canyon, I can tell you that sometimes, things don’t end well for base jumpers.) But, even day-to-day, we make risk-benefit decisions. If you woke up this morning with a headache, you very well may have taken aspirin, acetaminophen, or ibuprofen for relief. Each of those medications carries certain risks (you might be surprised at all the risks listed for them), but for most, I doubt they gave that much thought, and merely wanted the headache to go away. Some people probably woke up to snow and ice on their sidewalks and the streets. You make a risk-benefit in deciding whether to shovel your sidewalk (as a physician, I can tell you that during these times, we see an increase in heart attacks and falls with injuries) and you make a risk-benefit decision in deciding whether to venture out on the streets, realizing that even if you are a highly skilled driver on the ice, in my experience, not an insignificant number of drivers are totally incompetent to drive on it.)
I also indicated that your risk tolerance may very well change at different points in your life. Those of us old enough likely remember well our “immortal years” of youth when we were game for almost anything and often failed to perceive or give proper consideration to risks that we wouldn’t dare take today, and we probably try to impart on our children that they should not take those same risks. I also took more risks when I was single than once I became married, both because of my increased responsibilities I felt I owed to my wife, but also because one of the reasons God gives us a wife is to tell us “no” when we come up with lame-brained ideas we want to try. For me, it became even more so once I had kids. I took fewer chances when I knew that if I became disabled or died, I would not be able to provide for them and they might have fewer opportunities. I purchased disability and life insurance to mitigate that risk. When I shoveled snow as a kid, I had no reservations. Now, I wait until it is light out, I wear more appropriate clothing and shoes, and I keep a phone with me in the event of a fall. Also, I am much more willing to accept the assistance of my grandkids to shovel the sidewalk for me!
So, let’s now put ourselves in the shoes of that 30-, 40-, or 50-year-old, married man or woman, with a family early in 2021. Faced with the information that there is a 75 percent chance they will be involved in an auto accident in the next year, how might they think about the risk? First, of course, there might be a few who would look at it as a 25 percent chance they won’t and not take any measures, thinking that chances are that even if they are in the 75 percent, it won’t be a big deal, certainly not worth changing anything in their lives or routines. On the other hand, I do think that most people’s self-assessment of their risk of being involved in an automobile accident in the next year is far less than 75 percent, in fact, I would think most people would put that risk at less than a percent. So, being told that their risk for that next year is 75 percent, I suspect that would grab more peoples’ attention and at least concern them initially.
Probably, a lot of folks would think, okay, that is a high-risk, but I can reduce that risk by not riding in a car with someone I don’t know to be a safe driver, being extra careful and taking an extra look before I cross streets, and when driving, I will be sure to wear my seatbelt and stay at or below the speed limit. If I go out to dinner or a party and have some drinks, I will make sure to have someone else drive or call a rideshare service. Those would all be reasonable things to do.
There might be others who might be even more concerned. For example, if that person is pregnant or the spouse is pregnant, that might cause some to assess the risks as even greater and to want to take even more precautions, e.g., returning home earlier in the evening to avoid driving in the dark and others who may have begun their evening partying and potentially be driving impaired. It might cause them to limit their driving on a holiday weekend or evening when it can be expected that more people will be on the road and an increased number of them might be impaired. It might cause the family to reconsider a planned road-trip for that year. It would likely cause them at least some pause about venturing out in the car on snow and ice or other bad weather, especially with the pregnant person and kids in the car.
There might also be some who realize that a parent, a disabled child, or other is dependent on them, and if they were to become seriously injured, it would directly impact that dependent person’s life and well-being. That might factor into their risk tolerance.
I think that the risk analysis for any novel virus causing an epidemic or pandemic is in many ways analogous. If I told you back in 2021 that your risk of getting infected in the next year was 75 percent, I think there would be many analogous thought processes. Unfortunately, due to misinformation and disinformation, I suspect many did not appreciate the potential risks of infection.
Just as with the risk of an automobile accident, there would be some people who would think, well, there is a 25 percent chance I won’t be infected, and even if I am, chances are it will be the “fender-bender” or someone backed into my car- type of infection, that is to say, “mild.”
I think that a fascinating way our minds work is that in both cases, we tend to focus on the immediate risks and not factor in, or give much weight to consideration of less immediate consequences. For example, in an automobile accident, we tend to focus on did the person survive and was the person able to walk away from the crash. However, there are a whole host of injuries that can occur. Some of those injuries can require surgeries to address, others can cause significant pain for a protracted period of time, others can result in disability, and some of these could impact our ability to work for a period of time or even indefinitely. And, of course, even if you are in an accident and not seriously hurt, it still could be that someone else in your car was hurt, someone in the other car was injured, or almost assuredly, a motorcyclist or pedestrian involved in the accident was seriously hurt. There can be traffic citations and court dates, criminal liability, lawsuits, and of course, the accident can result in increased future insurance premiums, especially if you were found at fault.
So, too, with COVID-19, the overwhelming focus by the CDC and by the public was on mortality rates, as if the outcomes of infection were either mild illness or you died. In actuality, there were many people who experienced protracted illness, including Long COVID, and these folks tended to be middle-aged – the very group that I used for our analogy above. There were others who developed cardiovascular complications of their illness and some of these people died months to a year or more following the apparent recovery from COVID-19 and these deaths were attributed to heart disease or stroke, and not to COVID-19. The key point being that when people evaluate their risk tolerance, they seldom factor in these longer-term risks and their consequences, which can lead to understating the risk of the accident or, for purposes of our analogy, the infection.
Further, we often focus our risk-benefit analysis too heavily on the impact to us individually, and not give the due consideration to the risk to others. As mentioned above, while we might survive the accident with no or only minor injuries, what about our spouse, what about our kids, what about others involved in the accident, and certainly motor vehicle accidents can pose risks to an unborn infant, even when the mother is not seriously injured. Similarly, while the infection of one person in the family may be mild, it can still cause severe disease in another family member who contracts the infection from that family member.
The point of all of this is to demonstrate that we humans are generally not good at conducting true risk-benefit analyses. It is for this reason that prior to the COVID-19 pandemic, public health and medical professionals most often recommended the “precautionary principle;” that is to say that until the risks can be better known, people would be well-advised to use precautions to avoid infection. But when we dislike the risk mitigation measures that would be necessary to reduce the risks, we are much more likely to rationalize and reduce the risks in our minds and to others. For driving, most people would likely have no problem with wearing seatbelts and recommitting to following speed limits. When told that we have a 75 percent chance of being involved in some kind of motor vehicle accident, we might even be willing to think that we would return home earlier at night, at least until we are with friends and really enjoying ourselves and not wanting to leave. We might even say we would put off a planned road trip until the following year, at least until friends invite us to go camping, fishing or rafting with them.
So, too, many took steps to minimize exposure to infection early in 2020. That became more difficult as society progressively returned more and more towards normal activities and ceased implementation of many of the protections that it adopted in the first year of the pandemic.
We heard many promoting on social media and cable networks that the vaccines were not safe, and this or that happened to some people who were vaccinated, which is surprisingly a very effective scare tactic and deterrent to immunization. However, every one of those doctors promoting these messages that I read or watched never presented the risks in a balanced way, as often what they raised alarm about occurred far more frequently and far more severely in people who became infected rather than through vaccination. It is impossible to make a personalized risk-benefit analysis when you are manipulated by unbalanced information. For example, I can tell you that almost any cancer drug is not “safe.” If I was seeing you in my office and only told you about all the terrible side effects and adverse effects you might incur with the chemotherapy, but did not indicate that there was any benefit in treating your cancer, of course no one would agree to undergo that therapy. If I only tell you the good about a treatment or only tell you the bad about a treatment, then I am manipulating you to try to get you to make a certain decision about your treatment. That is not informed consent. That is unethical to the foundation of medical principles.
To complete our analogy, it would not have been unreasonable to tell someone in 2021 that we could expect about a 75 percent chance that they would become infected with SARS-CoV-2 sometime in the following year if they were out and about as is typical – work, school, grocery shopping, social gatherings, etc. and they utilized no other mitigation measures. There were a range of mitigation strategies people could choose from that would decrease their chances of exposure and thereby infection. Once infected, for most of 2021, there was little we could do until you were at the point of needing hospitalization to reduce the severity of your disease and try to avoid death (an antiviral for outpatients did not get emergency use authorization until December of that year).
Vaccines were the game changer for reducing the risk of severe disease and death. During 2021, especially with the delta variant, the rates of hospitalization and death were many fold-reduced in those who were vaccinated versus those who were not. The problem is that we had no way to identify who would get severely ill if infected, just as in the analogy, I could not tell the person whether the motor vehicle accident (if they were part of the 75 percent) would result in hospitalization or their death. In both cases, it was the minority of all infections and the minority of all motor vehicle accidents. It is probably worth pondering that I have talked to a lot of people who unexpectedly got very ill from COVID or who developed Long COVID; almost none of them thought that would ever happen to them. Similarly, you may know of people who survived motor vehicle accidents or friends or coworkers who had a seriously injured family member or lost a family member to a motor vehicle accident. It is likely that none of them expected that to happen that day as the family member got into their car.
So, I will leave you with a framework for decision-making when we face the next pandemic with a new virus and you need to make the decision for yourself as to whether to take precautions to prevent getting infected for as long as you can or to buy-in to what will undoubtedly be people suggesting that large numbers of people need to go ahead and get infected to develop herd immunity or perhaps making the argument that it is good to get infected to build up your immunity:
Look for trusted sources of information, e.g., the American Academy of Pediatrics, the American Society of Infectious Diseases, the American College of Physicians, CIDRAP (The Center for Infectious Diseases Research and Policy at the University of Minnesota).
Be weary of doctors who don’t express uncertainty; don’t admit to having been wrong about anything; use political or inflammatory language when seemingly trying to educate the public; and aren’t willing to provide clinical studies to support their positions.
If the novel organism belongs to the same family of viruses as ones we have experienced before, for example a coronavirus or an influenza virus, assume that the new virus transmits in the same ways as the known viruses do until proven otherwise. In other words, if there is an outbreak of a new coronavirus or influenza virus, assume that that there will be airborne transmission until proven otherwise and be skeptical of advice that recommends only washing your hands for infection prevention.
Keep in mind that no virus that has caused a pandemic in the past has built up our immune system.
Don’t buy in to any talk of herd immunity if you are hearing of reinfections occurring within a year.
Remember that because vaccines use weakened, killed or only parts of the infectious virus, any adverse effect that you might experience with vaccination would likely be far worse with natural infection.
Remember that your risk of more serious disease with infection with almost any organism will be greater if you have underlying health conditions, are immunocompromised, or are pregnant, and that the risk to the fetus is likely greatest in the first two trimesters.
Finally, you would be wise to consider the precautionary principle. Use extra precautions until the disease outbreak has fully unfolded and you can see what kind of illness it is causing and how severe it is.
Polio and other vaccines have been thrust into the spotlight with a New York Times report on December 13th that was updated on the 15th by reporters Christina Jewett and Sheryl Gay Stolberg revealing that an attorney working with Robert F. Kennedy, Jr. had petitioned the government to revoke (or suspend) the FDA’s approval of the polio vaccine (specifically, the vaccine with tradename IPOL for which the proper name is Poliovirus Vaccine Inactivated) for infants, toddlers and children. The article also indicted that RFK, Jr. has expressed interest in having this attorney serve in the U.S. Health and Human Services Department as general counsel to the organization that President-elect Trump has nominated RFK, Jr. to lead as cabinet secretary.
In the petition, the attorney argues that the basis for the request is that there were not properly controlled and properly powered double-blind clinical trials of sufficient duration to assess the safety of this vaccine.
It should be noted that this polio vaccine is the only polio vaccine licensed for use in the U.S.
Today, the globally available polio vaccines are generally referred to as IPV (inactivated poliovirus vaccine) and OPV (oral poliovirus vaccine). Though people my age will recall getting a “sugar cube” polio vaccine in elementary school, OPV is no longer approved for use in the U.S. (I will explain below), but OPV continues to be used through much of the world due to its lower cost and ease of administration (compared to IPV which is administered by injection).
Jonas Salk invented IPV and it underwent clinical trials beginning in April of 1954. One year later, the results showed that the vaccine was safe and effective, and the vaccine was licensed for use in the U.S. and many countries of the world. The oral polio vaccine was invented by Albert Sabin and licensed in 1961. It was subsequently licensed in 1963 in a trivalent form that would include all three serotypes (strains) of the poliovirus.
What is the poliovirus?
The poliovirus is an RNA virus that belongs to the family of picornaviruses and a specific group of these viruses referred to as enteroviruses, so named because they are transmitted through the gastrointestinal tract. Humans are the only known natural host for this virus, which likely explains the success of elimination efforts through vaccine programs.
As alluded to above, the virus is transmitted through the fecal-oral route (the virus is shed in the stool of those who are infected, which can then contaminate the person’s hands and be transmitted to another person through direct contact, who then ingests the virus and in turn becomes infected) and potentially an oral-oral route (virus can be present in saliva soon before and after the onset of symptoms). Thus, transmission often occurs with young children. Children can also shed virus in their nasal secretions. The period of viral shedding is several days to several weeks.
As mentioned above, there are three serotypes of poliovirus (meaning three distinct types or strains of the virus) that can cause disease in humans (and infection with one serotype is not protective against infection with another), cleverly named serotypes 1, 2 and 3. These also are sometimes referred to as wild type 1, 2, and 3 (meaning the form of the virus that originally occurred in nature). After a global eradication effort with vaccines, serotypes 2 and 3 were certified as globally eradicated in 2015 and 2019, respectively. As for serotype 1, as of 2020, it had been eliminated from every country in the world except Pakistan and Afghanistan.
What is polio?
Polio is generally the term used to refer to the disease caused by infection with the poliovirus. Though the disease can have quite a range of presentations and consequences, many people use “polio” to refer to the most severe form of disease that is technically referred to as poliomyelitis.
The majority of infections with the poliovirus do not produce symptoms or signs of disease (~72% of cases are asymptomatic). However, these children shed virus and can infect others. About 24 percent of infections in children cause mild illness characterized by fever, sore throat, headache, and in some cases, a rash. These symptoms generally resolve within a week.
Nevertheless, the virus replicates (divides to form more virus) in the oropharynx (throat and nose) and in the gastrointestinal tract, and from there moves to the tonsils, lymph nodes, and from there, the bloodstream. In most cases, the body’s immune defenses can contain the virus, but in some individuals, the virus will seed (meaning the virus lands there and hangs out) the spleen, bone marrow, muscle and other deeper and more remote lymph nodes. It is in these individuals that a second, much more significant amount of the virus can enter the bloodstream and, in these cases, the brain and spinal cord can be infected. When this happens, we most often see one of two forms of disease – nonparalytic aseptic meningitis (meaning an inflammation of the lining of the brain and spinal cord with fever, headache, neck stiffness, and back pain; but without paralysis and without virus detectable in the spinal fluid) or paralytic poliomyelitis. The nonparalytic form of disease generally will resolve completely over time.
Paralytic poliomyelitis is the most feared outcome of infection. We cannot predict who will develop this. These children (or sometimes adults) may not have any of the initial symptoms listed above for those with symptomatic infection, or they may have these symptoms and appear to be recovering when within the next days to weeks, they now experience fever, headache, muscle pains, and muscle spasms involving their limbs and back. Within 2 – 4 days, they may develop acute flaccid paralysis (meaning sudden weakness of the arms and legs that are just limp with no muscle tone). Fortunately, in most cases, the paralysis will involve only one side of the body, and more often the legs than the arms, however, in the most severe form, the paralysis can affect all limbs on both sides of the body and even the muscles required for breathing and swallowing (these are the cases frequently seen in “iron lungs” if they survived). [The case fatality rate (CFR) for paralytic polio is 2 – 5% among children and as high as 15 – 30% for adolescents and adults. The CFR for those with the most severe complete paralysis form of disease ranges from 25 – 75%.]
Only about 10 percent of those with paralytic poliomyelitis will experience a complete recovery, though those with one-sided paralysis and persistent weakness can improve over time. However, in a cruel twist of fate, anywhere from 15 – 40 years after seeming recovery or improvement, 25 – 40% of those who contracted paralytic poliomyelitis as a child can experience new onset muscle pain and an exacerbation of existing weakness or even new weakness or paralysis in another form of disease that we refer to as post-polio syndrome.
Prior to the availability of vaccines, polio disabled up to 21,000 people a year in the U.S. President Franklin D. Roosevelt was infected at age 39 and developed paralytic poliomyelitis. He continued to have weakness of both legs and used braces and eventually a wheelchair while in office as President of the U.S. Senator Mitch McConnell was infected at age 2 and developed paralytic poliomyelitis, predominantly affecting his left leg, but fortunately, recovered strength in that leg over time with physical therapy.
Inactivated Polio Vaccine
The clinical trial for the IPV was the largest clinical trial that had ever taken place in U.S. history – including 1.5 million children in 211 counties in 44 states- and far larger than we typically conduct for phase III clinical trials of vaccines today. In this study, 623,972 children received either the vaccine or a placebo (placebo controls), and the remaining more than 1 million children were observed with no intervention (observed controls). The vaccine was 80 – 90 percent effective in preventing paralytic poliomyelitis. Given by injection, the vaccine would not be expected to prevent infection from a virus that infected the gastrointestinal tract through ingestion, but on the other hand, there could be no shedding of virus in a vaccinee’s stool to potentially infect an unvaccinated close contact.
In more recent studies of IPV with our ability to measure neutralizing antibodies, 83 infants had detectable neutralizing antibodies 13 months following a series of three IPV doses of vaccine as follows: 97.6% (type 1), 100% (type 2) and 100% (type 3). For all subjects tested, titers of neutralizing antibodies rose at least 10-fold after 2 doses and at least 100-fold after 3 doses.
No subjects reported serious adverse reactions (one adult did report redness at the injection site). There were no significant local or systemic reactions. In children, fevers did occur following injection in 7% after the first, 12% after the second, and 4% after the third injection (note that most children received their DPT vaccine dose at the same time, and reported similar proportions with fevers after receiving DPT vaccine only.
The results were a dramatic decrease in cases of paralytic poliomyelitis following use of this vaccine (and about six to eight years later the use of OPV). The last case of paralytic poliomyelitis in the U.S. from wild type poliovirus was in 1979.
It makes no sense to suspend or end the use of IPV to conduct more studies as requested by RFK, Jr’s attorney. First of all, the vaccine has been in use in the U.S. for 69 years. Almost every living American was immunized with IPV, OPV or both. If the vaccine has safety events even in the range of 1 in 100 million people, we would have seen those safety signals by now. And, of course, there can be no better evidence of vaccine effectiveness when an infectious pathogen has been eliminated from the U.S. following the vaccine campaign. The only cases of polio that we see today are from unvaccinated or immunocompromised individuals being infected with wild type virus from travel to another country, or an unvaccinated or immunocompromised individual being infected by someone from another country travelling to the U.S. and shedding the vaccine derived virus in their stools. Even the most hardened vaccine cynic who is convinced by none of the above would have to admit that the levels of polio disease detected in the U.S. are so low as to make a clinical trial now impossible to assess vaccine effectiveness. Perversely, the only way to retest vaccine efficacy now would be the requested nationwide suspension of use of polio vaccine to allow polio disease to return to levels that would allow for the proposed clinical trial. However, that would lead to a senseless and dramatic rise in polio cases and associated disability, which I cannot imagine would pass the ethical review of any study committee, especially when no reputable virologist, immunologist, physician, or public health official has made a serious argument questioning the safety or efficacy of IPV.
Oral Polio Vaccine
The OPV appears to be similarly effective to IPV, however there are some important differences in these vaccines:
The OPV is administered by mouth instead of injection.
The OPV contains weakened strains of poliovirus that are not able to cause neurological disease, but do cause a low-grade infection of the gut, whereas the IPV contains inactivated virus that cannot replicate and cannot cause infection.
Persons who receive OPV can shed these weakened polioviruses in their stool and can infect unvaccinated close contacts. Because IPV is given as an injection, there is no shedding of the vaccine virus and the vaccinated person poses no risk to others.
Because the weakened polioviruses are designed to infect the gut in order to create the immune protection, this vaccine should not be given to immunocompromised individuals, whereas IPV is safe in this regard for persons who are immunocompromised. In about 1 in every 2.4 million people who receive OPV, in the process of infecting the gut, the virus can revert to the form that can cause neurological disease and the vaccinated person can develop vaccine-associated paralytic polio.
For all these reasons, the U.S. discontinued the use of OPV in 2000 because polio elimination had been so successful that a person, although extremely rare, would now be more likely to develop paralytic poliomyelitis from the OPV vaccine than from wild-type virus.
However, many countries of the world use OPV for their vaccine responses to polio outbreaks. In Pakistan and Afghanistan, it is very difficult to administer injectable vaccines throughout the country, and at times, the necessary health care professionals needed to administer injections have been targeted. OPV is a less expensive and much easier option to distribute, especially to remote areas of a country. However, for the same reasons as above, if someone receives OPV in another country and then travels to the U.S., they may be shedding the vaccine virus and this would pose a risk to unvaccinated Americans, as unfortunately happened to a young man in New York state who is now paralyzed.
Other than sanitation (especially clean water, proper food handling, and reducing human exposure to rodents), I cannot think of anything that has done more to reduce childhood mortality, relieve human suffering and extend human life expectancy than vaccines.
What is a vaccine? In general, a vaccine is something given by mouth (e.g., polio vaccine), intranasally (e.g., one version of the flu vaccine), or by injection (the majority of vaccines) that exposes the body to a part (e.g., a protein) or the whole (but an inactivated or weakened form) of the organism that causes the disease that the vaccine is intended for such that the body will then mount an immune response (primarily antibodies, but it can be much more than that) that will be protective to some degree when the vaccinated person is later exposed to that infectious threat.
Why do vaccines make such a difference to our public health?
Let me start with a disclaimer. This particular blog post is intended for readers who don’t understand anything about vaccines, immunology or infectious diseases. Therefore, I will necessarily have to oversimplify my explanation. There are many nuances to all of these subjects, and I am not going to explore these. In fact, I am going to try to avoid as much medical jargon and as many technical terms and concepts as possible. To do so, I am going to largely use analogies. Like all analogies, they can help people understand general concepts, but they inevitably have their limits in that when carried too far, the analogy always begins to fall apart.
So, here we go. Imagine that you are the head of Homeland Security for the U.S. You are informed that our intelligence agencies have identified a threat of attack on our homeland within the next six months with a moderate degree of confidence. The problem is, the agencies are not yet certain of the type of attack, the number of people involved in the planned attack, the identities of any of the potential attackers, or how they plan to enter the country.
This head of Homeland Security is going to be our analogy for you back in 2021 as we were in a pandemic and you knew that there was this invisible virus out there awaiting to attack and invade the bodies of those who were susceptible to infection (which was almost everyone).
Of course, one approach that the head of Homeland Security could take is to realize that we already have many systems in place to thwart entry into the U.S. by potential terrorists and to prevent potential attacks, such as our passport system, our no-fly lists, TSA and their security measures, the Coast Guard, the Border Patrol, various security check-points, the U.S. Postal Service and a host of other security measures, and to feel confident that chances are, the potential terrorists could not evade all of these measures. And, the director might assume that even if one or more of the terrorists did get through, the likelihood is that any attack would be relatively minor and local in nature. Similarly, this is the decision that many during the pandemic made in declining the vaccines, realizing that even though we had no idea as to who might be carrying the virus and end up infecting us, that we have many systems in place to protect us from attacks by viruses, and that even if the virus was successful in infecting us, the chances were that the illness would be mild and limited.
Many of us might not have the same degree of confidence as that director of Homeland Security given that sophisticated terrorist networks evolve. They learn from past mistakes and they learn where the obstacles in our system of barriers and protections are and how to potentially get around them. So too, viruses evolve. Certain types of viruses (RNA viruses – a group that includes the influenza virus and SARS-CoV-2) evolve faster, and the larger the number of humans they infect and the larger the number of species of animals that they infect, the faster and more dramatically they evolve. Just as terrorists learn how previous attacks were stopped, viruses “learn” how our immune systems are blocking them, and they may develop ways to get around those immune defenses. It is unlikely that viruses will acquire the ability to defeat every one of our defenses, but just as for terrorists, they don’t have to in order to inflict a great deal of harm. Even with our most horrific domestic terrorist attack on 9/11, the terrorists didn’t evade every line of our defenses – one of the attacks was thwarted by our last line of defense: regular Americans who were passengers on the plane and who bravely overtook the terrorists at the cost of their own lives. Similarly, when we are exposed to a virus, it is not a single virion, but generally hundreds, thousands or tens of thousands. Many of those virus particles will be stopped in their tracks before infecting us, but it only takes a small number of successful virus particles getting through these defenses and infecting cells to cause potentially serious harm.
Although I have no law enforcement or national security experience or expertise, I would imagine that most directors of Homeland Security would not want to take the chance that our current routine barriers to entry and processes would catch all of the potential terrorists before they could enter the U.S. (In the analogy, the terrorists are the SARS-CoV-2 virus and the U.S. is our body consisting of cells which the virus can infect if it gains entry.) I imagine that one piece of information that would be critically important to the director in an effort to thwart this planned attack would be to know by what route the terrorists plan to enter the U.S. – land, sea, air – so that barriers to entry could be enhanced. Using our analogy, though we didn’t know who was carrying the virus and would be a threat to us (because at that time our testing was inadequate and because we knew that a substantial number of people that were infected and contagious were asymptomatic and didn’t realize that they might be contagious), we did know how the virus planned to enter our bodies – through aerosols that we breathe in through our nose and mouth. Thus, for those who wanted to enhance their defenses against virus particles trying to invade by this respiratory route, there were a number of interventions that could be used – e.g., increasing ventilation indoors; utilizing air purifiers and air filters; avoiding large numbers of people in poorly ventilated spaces; physical distancing; and utilizing well-fitting, high-quality masks.
I would suspect that another critical piece of information for the director besides the route by which the terrorists plan to enter the country would be to have the identification of the terrorists and a description of each. That would allow our surveillance and security checks to be far more focused and decrease the potential for a terrorist to slip by undetected. Having their descriptions would be great; images would be better; and having their finger prints and DNA would give us positive identification, especially in the case that we were able to make a preemptive attack on the terrorists before they could attempt their attack on us.
So, too, if our bodies have a description of key distinguishing and identifying features of the virus that threatens us, our immune systems can be better prepared, can respond much more quickly and precisely, and we can have a better chance of stopping more of these potential invaders at our border before they can infect our cells. That is what vaccines do. They give us a relatively harmless piece of the virus (e.g., the spike protein in the case of the COVID-19 vaccines) or a “killed” or inactivated entire virus that allows our immune systems to learn to recognize this potential invader much like having the virus’ image and fingerprints, and enable the immune system to respond much faster the next time the body is exposed to that invader.
That faster response helps prevent serious illness in a number of ways. One way is that when antibodies are already preformed against the invading virus, the antibodies have the potential to “neutralize” the invading virus – i.e., prevent the virus from ever invading a cell and causing infection. Once virus enters a cell, the antibodies no longer have a way to get to the virus until the virus has replicated many times over and leave that cell to invade other cells. Just like an invading army, it is much easier to stop a team than a squad of soldiers, and much easier to stop a squad than a platoon, and so on, and much easier to defeat the invaders before reinforcements arrive. Thus, when antibodies are at the ready, fewer invading virus particles will get through and invade cells. Once in cells, the invading virus particles get thousands or hundreds of thousands of new virus recruits that are made in the cell and released to infect other cells. Thus, the more virus particles that are stopped before they are able to infect and reproduce inside cells, the lower the total number of infecting virus particles (we refer to this as viral load), and for many infections, viral load has some correlation to severity of illness. So, while many people might be able to rely on the normal defenses that are already in place and might have only a mild illness as the result of an infection, vaccines greatly increase and enhance the defenses and increase the odds that the illness will not be severe. We saw this over and over again in hospitalized patients with COVID-19 – those requiring hospitalization, those requiring critical care, and those dying from COVID-19 were many times more likely to not have received the vaccine.
To return to our analogy, let’s say that the director now becomes aware of intelligence identifying the location of the terrorists who are planning the attack on the U.S. They are meeting in a building in an urban center of another country. Unfortunately, it is still not known precisely who the terrorists are or how many there are. Bombing the building would be sure to take the terrorists out and prevent the attack on U.S. soil, but would also be sure to cause much collateral damage in terms of economic damage, injuries and loss of innocent lives, not to mention political fall-out. A more targeted approach – a raid of the building, a room-to-room search, and detaining of individuals until it could be determined whether they are one of the terrorists would be highly risky and difficult since the identities of the terrorists are unknown.
In the case of SARS-CoV-2 infections, a similar dichotomy exists once a would-be virus invader has been sensed. The part of our immune system that is on guard for invaders before antibodies are developed can only detect that the invader is different from things that are normally part of our body, and instead of the precision-targeting of the invader like a sniper would perform, it must resort to releasing all kinds of chemicals (chemokines, cytokines among them) and responses that are analogous to firing a tank, dropping a large tonnage bomb, or throwing a grenade at the invaders. Like the option of the director in recommending to the President that the building housing the terrorists be bombed, this non-specific response will often at least slow down the virus invaders, but also cause collateral damage – e.g., injuring nearby cells and tissues and causing uncomfortable symptoms.
The extent of this exaggerated, non-targeted response is also often related to how similar the invading virus is to prior viruses that the person has been exposed to. For example, the SARS-CoV-2 virus was what we called a “novel” virus, meaning that as far as our immune systems were concerned, the vast majority, if not all, people were unlikely to have any preexisting immunity to this virus. The same thing happened in 1918 with the pandemic Spanish flu [A(H1N1)] virus. In both cases, the viruses were novel and in many, especially children in the case of SARS-CoV-2 and young adults in the case of the Spanish flu, the body responded to the infection with what is called “cytokine storm,” an exaggerated release of chemicals disproportionate to the direct threat of the virus that itself did more damage than the virus and caused organ damage to the patient, sometimes resulting in death. Vaccines do not only improve the immune response by having antibodies at the ready for a much faster response and potentially diminishing the viral load resulting from infection; in some cases, and this appears to be the case for COVID-19, they moderate the immune response significantly decreasing the chances that someone will develop cytokine storm.
I am often asked whether our seasonal flu vaccines could be used to prevent avian influenza (bird flu) infections, and if not, how long would it take to produce and distribute bird flu vaccines. I’ll try to answer both questions in this blog post.
The U.S. government has stored some H5N1 vaccines made in the early 2000’s in our Strategic National Stockpile. That is good, and even better news is that though those vaccines were designed based on three different clades (think strains) that were circulating in Indonesia and Vietnam at that time, tests have shown that these vaccines produce neutralizing antibodies (these are the antibodies that prevent the virus from infecting and entering our cells) to the clade that is currently circulating in the U.S. dairy cattle. The bad news is that there is not nearly enough vaccine were it to be needed.
The government does not disclose the actual inventory in our Strategic National Stockpile, likely for good reason. So, I can’t tell you exactly how much H5N1 vaccine is in the stockpile, however, the limited public reporting suggests that it is a number in excess of 10 million doses, but less than 50 million doses.
How much vaccine would be needed? Assuming that everyone in the U.S. would be eligible (however, none of the currently approved vaccines are approved for children less than 6 months of age), that would be 326.7 million people. All of the currently approved vaccines require two doses to be fully vaccinated. That would require 653.4 million doses of vaccine, less an estimated deduction of 6.4 million doses for children less than 6 months of age who likely would be ineligible for a new total of 647 million doses needed. Of course, there will be many people unwilling to get vaccinated for a variety of reasons, largely because we can expect a significant vaccine disinformation campaign, but as I frequently say, there are no rabies vaccine antivaxxers since the mortality from rabies is 100 percent in the absence of post-exposure vaccination. I would anticipate that vaccine uptake would be higher for avian influenza than for COVID-19 because the case fatality rate is expected to be markedly higher (30 – 50 percent for avian influenza versus 1 – 3 percent for COVID-19) and unlike COVID-19, there is reason to believe that children would be more severely impacted than older adults.
In the most recent year (2023 – 2024 influenza season) for which data is available, approximately 55 percent of children ages 6 months through 17 years received the annual flu vaccine and approximately 45 percent of adults were vaccinated. One would imagine that interest in the avian influenza vaccine would be even higher if we were facing an imminent pandemic threat, but even if we just go with a conservative guess that 50 percent of Americans ages 6 months and above would want the avian influenza vaccine, that would now result in the number of doses of vaccine needed to be 323.5 million.
If we take the high end of the suspected number of vaccine doses in the current U.S. stockpile (50 million), that still leaves a gap of 273.5 million doses. In May of this year, the U.S. Department of Health & Human Services indicated that it was obtaining an additional 4.8 million doses of vaccine that is more targeted to the current H5N1 clade circulating in the U.S. as opposed to the vaccines in the stockpile that were targeted at earlier clades circulating in Indonesia and Vietnam. Those doses were expected to be delivered this past July, but still need to go through the FDA’s approval process. I don’t know whether these vaccines were included in the estimates of the stockpile reserve or not, but if we assume the most optimistic case, that now only reduces the gap in needed vaccine doses to 268.7 million.
In the egg-based production process of influenza vaccines, the influenza virus that we want to design the vaccine for is injected into fertilized chicken eggs and incubated for several days to allow the viruses to replicate. The fluid containing virus is then obtained from the eggs. For inactivated influenza vaccines (which all of the currently approved H5N1 vaccines are), the vaccine viruses are then inactivated (killed), and the virus antigen is purified. The manufacturing process continues with quality testing and review by the FDA, packaging and distribution. This process can take upwards of 6 months from start to finish.
Since 2012, there is a new way that influenza vaccines can be produced called cell culture-based production in which the CDC supplies the influenza virus for the vaccine (in this case an H5N1 virus) to the vaccine manufacturer, who in turn inoculates mammalian cells with the virus in culture and allows the influenza virus to replicate for a few days. Then, the virus-containing fluid is collected from the cell cultures and the virus antigen is purified. The manufacturing process continues with purification, virus inactivation, and testing. Finally, the FDA tests and approves the vaccines prior to release and shipment. Since the 2021 – 2022 season vaccines, those made by this method are entirely egg-free and thus safe for those with egg allergies. The advantage to this methodology is that it does not require fertilized eggs, which could be a very big deal because in an avian influenza epizootic (epidemic among animals), poultry are generally involved and our only current way to manage those outbreaks is to cull all of the poultry on that farm. Obviously, when these outbreaks are occurring throughout our country, this will result in a decrease in supply of chicken eggs. Also, because it is easier to come by the mammalian cells than fertilized eggs, this process can be completed a bit sooner than the egg-based production of vaccines.
The point of all this is to state that as of right now, we don’t have near enough vaccine to respond quickly to an avian influenza epidemic. Current avian influenza vaccine contracts between suppliers and the government would increase the supply by another 10 million doses, but that vaccine is not scheduled for delivery until the spring of next year. Projections are that in the event of an emergency, 100 million doses could be produced within 5 months. At this rate, it would take nearly a year and a half to produce all the needed vaccine (and recall that I built my estimated need for vaccine based upon roughly half of Americans wanting to get vaccinated).
Our only hope for a faster response would have to include mRNA vaccines, which can be produced much faster than either egg-based or cell culture-based current production methods. Of course, we are also at a time when we are undergoing a transition in presidential administrations. One of the President-elect’s closest advisers on health is a long-time antivaxxer. We also know that there is a movement afoot to try to prevent Americans from having access to mRNA vaccines based on rampant disinformation in large part spread by discredited doctors. If these efforts are successful, and I doubt they will be, we would obviously be seriously hampered in any effort to respond quickly to an emerging bird flu pandemic. The other reason that mRNA vaccine technology may be critical is that avian influenza viruses mutate frequently. Further, as I have previously written, we are entering into the human flu season and this greatly increases the risk for reassortment events, which could significantly alter the effectiveness of current vaccines. Without mRNA technology, a need to change the vaccine formulation to account for antigenic changes in the virus would set back the manufacturing process significantly.
Currently approved H5N1 vaccines:
Arepanrix – Influenza A (H5N1) Virus Monovalent Vaccine, Adjuvanted. It was approved on November 22, 2013 and is approved for those ages 18 years and older. It is produced using our traditional egg-based technology. The vaccine is given as two injections given 21 days apart. It was made by a subsidiary company of GlaxoSmithKline Biologicals (GSK), but it is not commercially available. Vaccine was produced for purchase by governments for their stockpiles. Last month, the FDA approved its use in children over 6 months of age.
Audenz – adjuvanted influenza A (H5N1) monovalent vaccine. This vaccine was approved in January of 2020. Production of this vaccine utilizes cell-based technologies, rather than egg-based. Audenz is given as a two-shot series 21 days apart. It also is approved for those ages 6 months and older.
Sanofi Pasteur produced an H5N1 vaccine solely for the Strategic National Stockpile and therefore, it has no trade name. It was approved by the FDA in 2007. It is an inactivated, monovalent vaccine for injection and approved only for those ages 18 years and older. It also is given as a two-shot series, but at an interval of 28 days apart. This vaccine is produced by egg-based technologies.
Now, I turn to the question as to whether our seasonal (annual) influenza vaccines might effective in protecting us from avian influenza. Until recently, I would have said not likely. However, this paper 36492242, was just posted online last week. This is an observational study in which sera from people born between years 1925-1967, 1968-1977, and 1978-1997 [if you are curious as to why these birth cohorts were chosen, it was to determine whether the immune responses of the age cohorts might be affected by the different influenza viruses that may have primed their immune responses. There were influenza pandemics in 1957 (H2N2), 1968 (H3N2) and 2009 (H1N1). The first cohort would have lived during the 1957 pandemic and likely primed by exposures to H1N1 (in circulation from the 1918 pandemic) and H2N2 viruses. The second cohort would have lived during the 1968 pandemic and thus may have been primed by exposure to the H3N2 virus. These different exposure histories might affect any cross-reactivity to the current novel H5N1 virus.] were collected before vaccination with 2021-2022 seasonal flu vaccine, 28 days following vaccination and 6 months post-vaccination with an inactivated seasonal influenza vaccine (i.e., the same seasonal flu shots most of us get). Then, haemagglutination inhibition, viral neutralization, and immunoassays were performed to assess the baseline protective immunity of the population as well as the ability of seasonal influenza vaccines to induce protective responses.
The investigators found that subtype-specific serological protection against H5N1 in the representative Spanish population evaluated was limited or nonexistent. However, seasonal vaccination was able to increase the antibody titers to protective levels (a caution here – we don’t know what level of neutralizing antibodies is required for protection against H5N1 infection, but the investigators made a reasonable assumption that it would be similar to the level required for other influenza A viruses, so the conclusion is likely incorrect if the assumption is incorrect) in a moderate percentage of people, probably due to cross-reactive responses. These findings demonstrate the importance of vaccination and suggest that seasonal influenza vaccines could be used as a first line of defense against an eventual pandemic caused by avian influenza viruses, to be followed immediately by the use of more specific pandemic vaccines (i.e., a specific H5N1 vaccine). This is a very important finding as it suggests that we may be able to buy some time while we are waiting for H5N1-specific vaccine to be produced by vaccinating people with the seasonal flu vaccines. In this study, that protection was lost by six months, so this may be a bridging strategy, but not a long one, or alternatively may require boosting, although that was not tested in this study.
The world’s population as a whole (I qualify this because there are some regions of the world that have experienced H5N1 outbreaks and survivors would be expected to have some degree of protection) does not have prior exposure to H5 nor preexisting H5-specific antibodies. However, there is more antigenic similarity between H1 (that we are regularly exposed to through infection and/or vaccination) and H5 than there is between the two hemagglutinin proteins that cocirculate each flu season in the U.S. (H1 and H3).
The neuraminidase (N) protein is also capable of stimulating an immune response and the production of neutralizing antibodies. While this study did not confirm this, perhaps because neither Spain nor the U.S. were as strongly impacted by the 2009 H1N1 pandemic as other countries, some have postulated that people who were infected with that pandemic virus, and perhaps those who were vaccinated with the 2009 pandemic virus, may have greater cross-reactive protection from antibodies specific to the N1 protein, and this may explain why we generally see more severe disease in younger people compared with older individuals. While neither the U.S. nor Spain were hard hit by the 2009 pandemic (thus, any cross protection that may exist may not exist in the majority of Americans), the U.S. did have more infections than Spain, and therefore, while protective antibodies were not detected among this Spanish population, it is possible that some Americans might have these. The N protein antigen is minimal in the inactivated vaccines, and thus N1-specific antibodies may not be significantly recalled after vaccination, however, it is possible that the live, attenuated nasal vaccines, which have been shown to induce stronger cell-mediated responses to N proteins, could be an option and this is worth studying to determine whether an increase in protection might be obtained from these vaccines in the short-term to help protect the population until more specific vaccines can be produced and distributed.
In the meantime, we need to continue research in this area. One exciting possibility is a “pan” influenza vaccine in early clinical trials that could include all the known hemagglutinin antigens of avian and human influenza viruses that might give us even better protection until a specific targeted vaccine could be produced and distributed.
My co-author and I wrote a book https://www.press.jhu.edu/books/title/12896/preparing-next-global-outbreak to capture the learnings from the COVID-19 pandemic because we were convinced that it did not serve as the wake-up call that it should have and that memories would be short-lived. In fact, we saw how the global outbreak of MPox shocked the world in 2022 – 2023, even while we were still combating COVID-19, and now we are witnessing a painful reminder that unfortunately, we were right as we watch the U.S. government fail to contain an outbreak of bird flu in cattle and poultry that is spreading to humans.
I have written several previous blog pieces that provide readers with the basics about avian influenza viruses and the developments in this outbreak. This blog post will provide an update on some concerning developments. I’ll state at the onset that I don’t know whether the avian influenza A(H5N1) virus spreading in dairy cattle will develop into a pandemic, but I can state this: Continued failure to contain this epizootic disease (essentially, an epidemic in animals), to take more aggressive steps to understand the mechanisms of transmission of the virus from animals to other animals and from animals to humans, and to increase testing and surveillance of disease transmission to humans is increasing the odds in favor of whatever chance there is for this virus to develop pandemic potential.
A quick review of some of the developments I have previously written about that are of concern:
Reports from public sources suggest that the virus has changed based upon what we have observed with more recent infections among California dairy herds:
The virus has appeared to become more virulent in cattle. Previously, what little data has been shared suggested that the case fatality rate among dairy cattle was less than 2 percent. That fatality rate among California herds has been reported to be in the 10 – 15 percent range.We were previously led to believe that the infections in other states resulted in a week-long, or perhaps two, of mild illness in dairy cows. Now California cattle are reported to often be sick for several weeks.
While we were led to believe that recovered cattle seemed to be completely recovered in other states, a California veterinarian stated that the recovered cattle seemed to only recover about 60 – 70 percent of their milk production.
It is also possible that the transmissibility of the virus has changed:
A California veterinarian estimates that as much as 50 – 60 percent of the cattle in the herds with these outbreaks are clinically ill, whereas previously, we were given the impression that isolation of infected cattle had contained the spread of infection to a small percentage of herds, perhaps on the order of 10 percent.
I also reported on a recent study that demonstrated that the virus obtained from an infected farm worker in Texas was able to transmit through respiratory droplets, although not hugely efficiently, in animal models, and that the virus was capable of infecting human lung cells.
Another concern of recent is the detection of the virus in pigs. The introduction of H5N1 into pigs increases the risk for genetic reassortments. Reassortments can occur when an animal is infected with two or more different influenza viruses. Pigs are hosts for both avian and human influenza viruses. We are also entering into the human flu season. If wild birds or cattle or poultry transmit H5N1 virus to pigs, and humans transmit H1N1 or H3N2 (our seasonal viruses) to pigs, the coinfection, which pigs seem to tolerate well, allows for the two viruses to swap entire segments of their genetic material with each other resulting in a novel virus that could acquire enhanced ability to transmit to humans, and even more concerningly, perhaps the ability for enhanced transmission from infected humans to non-infected humans.
So, where are things now?
The spread of infection is uncontrolled. In the U.S., for 2024, there are now (as of 11/5 for some of the data, and 11/8 for others):
51 jurisdictions with bird flu detected in wild birds;
Confirmed H5N1 in 10,528 wild birds;
48 states with outbreaks among poultry;
105,197,601 poultry affected by outbreaks;
15 states with outbreaks among dairy cattle;
443 diary herds with outbreaks of H5N1 infection;
46 confirmed human cases (25 related to cattle exposures; 20 due to poultry exposures (there was one additional case related to poultry culling in Colorado in 2022 that is not included in this number); and 1 case from Missouri for which no potential exposure has been identified. There are an additional 4 suspected, but not confirmed, cases.
Remember, each infection allows for the risks of mutations and the potential for the virus to develop enhanced transmissibility to mammals. As the human seasonal flu season begins, the risk for reassortments would be expected to increase.
While the human infections to date in the U.S. have been “mild,” it has just recently been reported that a teenager in British Columbia, Canada has been hospitalized with H5N1 infection, and there are unconfirmed reports that the child is requiring intensive care, though we have not been provided with any clinical details of the case. There are many concerns associated with this case:
Though we have no clinical details, it would appear that this child must be sicker than the illnesses previously reported in the U.S. given the presumed need to hospitalize the child and the unconfirmed report that the child is in intensive care. [The question this raises is whether the strain of the virus acquired by this child had undergone genetic changes that allowed the virus to infect the child’s lungs as opposed to the limited eye infections that have been reported in the U.S. The results of genetic sequencing of the virus have not yet been made available.]
No source of infection has yet been identified, or at least not yet reported. [The significance of this is whether the infection is a result of zoonotic spread (animal -> human) or whether there is undetected human-to-human spread. Thus far, no clear evidence for the latter has been identified, however, if that were to be the case, the pandemic risk would significantly increase.]
Finally, when the CDC conducted serology (antibody) testing of dairy farm workers, 7 percent were positive confirming that the number of infections are much greater in number than detected, and that many infections go undetected. https://www.cdc.gov/mmwr/volumes/73/wr/mm7344a3.htm. There are a few limitations to this study. First, it was conducted in two states (Michigan and Colorado), and thus, these results may or may not be translatable to what we are seeing in California. Given the data coming out of California, similar testing needs to be conducted in that state given the apparent changes to the virus virulence and potentially to transmissibility. Further, testing was limited to farm workers, so we cannot rule in or out potential forward transmission to family members or other close contacts.
It is notable that only 40 percent of those testing positive for H5N1 antibodies recalled having an unexplained illness. While there is no evidence to date that any of these farm workers were able to transmit the infection to anyone else (though in fairness, we really haven’t looked), recall that asymptomatic spread of disease is something that makes control of an outbreak much more difficult to control, as we saw first-hand with COVID-19.
It is also notable that only one farm worker was known to have worked with an infected cow. The implication is that cattle that were not clinically ill or identified as ill were able to directly or indirectly (e.g., through milking equipment) to transmit the infection to workers. This means that control of the outbreaks will be more difficult and that isolation of infected cattle will not be enough.
Finally, it was notable that none of those infected reported use of PPE, thus the one piece of good news is that we have every reason to believe that PPE will remain effective in controlling human infections among dairy cattle farm workers. On the other hand, the challenge is how to get workers to utilize it.