In my prior blog post on Why Get Vaccinated and How Do Vaccines Work, I tried to explain what vaccines are, how they work at a very basic level, and the benefits of vaccines that might weigh in favor of immunization for those who have no or only a rudimentary understanding of vaccines, immunology and pathophysiology. I used analogies to try to give the reader a clear and better understanding of these concepts at a very superficial level.
In this blog post, I once again am going to use analogies in order to give the reader a possible conceptual framework for being able to weigh the risks of getting vaccinated versus getting natural infection in the context of a novel virus, like SARS-CoV-2. And, like in the prior post, we will go back to 2021 – a year into the pandemic with this novel virus and the time at which vaccines were being rolled out. I want to point out that this risk-benefit analysis that we are going to go through would be quite different than the one for a routine childhood vaccination that has been in use for decades or the risk-benefit decision for hopefully rare situations such as a rabies exposure or even the risk-benefit decision for a vaccine against a potential, but unlikely future infection (e.g., certain vaccines for international travel), and I am not going to address these situations in this post.
For this analogy, we will again go back to the beginning of 2021. The COVID vaccines were just being rolled out. We knew that SARS-CoV-2 was quite contagious and that it could be transmitted by people who were asymptomatic or had mild symptoms that they may have attributed to allergies or other noninfectious causes, and therefore, those persons might be at school, at work or guests in your home without knowing that they were infected and contagious. We also knew that older individuals, obese individuals, immunocompromised individuals and those with certain underlying chronic medical problems seemed to be at greatest risk for severe disease (low oxygen levels, the need for hospitalization, the need for critical care, or death). We were starting to observe mutations that appeared to enhance the transmissibility of the virus.
One of the most disappointing things to me was that we were also seeing a growing number of reports of reinfection, meaning that we could not count on an infection conferring long-term, durable protection from reinfection. At that time, we did not know the consequences of repeated infection, however, we had begun clinical studies to try to understand why some patients who survived COVID-19 had lingering illness (Long COVID) that in some cases was quite disabling to the patients, and in many cases delayed a return to work, prevented a full-time return to work, or in some cases patients were no longer able to perform their job duties.
The clinical trials of the two mRNA vaccines that were the first to be available in the U.S. had included 43,548 participants in the Pfizer vaccine trial (21,720 received the investigational vaccine, 21,728 received a placebo and served as the control group) and 30,420 participants in the Moderna vaccine trial (15,210 in each group). A serious adverse event occurring once in every 100 people would be a rate of 1 percent. So, both trials were designed to detect any common serious adverse events. If a serious adverse event occurred at a rate of 1 in every one hundred thousand or 1 in every million people, obviously, those might not show up until the vaccine was rolled out to the general public.
So, now let’s go back to early 2021. Vaccines are being rolled out. Vaccination of health care professionals and first responders had already begun. The elderly now would be able to sign up to get vaccinated and then the roll-out would continue to other groups. If you were a 30-, 40- or 50-year-old, married adult with kids and a spouse, in reasonably good health, but lets say a bit overweight and perhaps some mild hypertension controlled on medication, how might you think about whether to get vaccinated.
Let’s say that I told you at that time that during the next twelve months, there was a 75 percent chance that you would be involved in an automobile accident. What I can’t tell you is whether it will be a fender-bender; someone will just back into your car or vice versa; you will veer off the road and collide into a tree or your car end up in the river; your car will roll-over or be totaled and if so, whether you will escape unscathed, be killed or survive, but have multiple broken bones, a concussion or perhaps even lose a limb or be paralyzed; or whether it will be an auto-pedestrian accident in which you might be the driver or the pedestrian. I also cannot tell you whether you will be alone or have someone else in your car who will be harmed or not. I also cannot tell you whether you will be the driver or the passenger in the car.
[I picked the 75 percent number because in our analogy, the automobile accident is the analogy for getting COVID-19. At that time, we did not know what a person’s chances were of getting infected in the upcoming year, however, we know that by the end of that year based on antibody testing, roughly 75 percent of children and adolescents had been infected at some point during the pandemic, and possibly more than once. This is a good group to use for this analogy, because this is the group for which there were the fewest mitigations undertaken, and so, it is not unreasonable for us to use this as our baseline risk with no mitigations (working from home, avoiding large gatherings, physical distancing, having good ventilation, masking, etc.) for the adults in our analogy, especially because school-aged children are often the ones who are the index case (first infected) for spread of infection in a household. Now, in fairness, Dr. Marty Makary, the current nominee to lead serve as the FDA Commissioner for President-elect Trump wrote a Wall Street Journal op-ed published in February 2021 that we would achieve “herd immunity” by April, a prediction that some people may have in part relied on to decide against getting vaccinated early in 2021. However, as I mentioned above, in observing the increasing number of reinfections, I was telling people and writing in my book that herd immunity was very unlikely because we are not seeing durable individual immunity – a prerequisite for herd immunity. For purposes of this analogy, I am not going to factor that some people were likely duped by Dr. Makary’s article in believing that vaccination would be unnecessary because (1) it was obviously proved to be wrong even relatively early in 2021, (2) by that time, we were already seeing clear evidence of new variants emerging (alpha and beta by this point in time) that demonstrated that the virus was evolving and actually becoming more transmissible and likely immune-evasive, and (3) as I mentioned, we were still not seeing evidence of long-lasting, durable immunity from infection, without which herd immunity is not possible other than potentially with vaccines.]
So, if I told you about your 75 percent chance of being involved in an automobile accident in the coming year, what might you do differently? A lot of the answer depends on your “risk tolerance.” We all take risks every day. People have different tolerance levels for risk at different points in their lives and in part, based upon their life experiences (e.g., many who have never done so might fear sky diving and think about all kinds of risks that might come to fruition, where as someone with much experience and confidence might assess the risks as being much lower and very willing to do so. Even fewer might be willing to go base jumping (jumping off buildings, cliffs, or bridges with a parachute) and, I imagine that even many who might assess the risks of sky diving to be minimal, might be unwilling to accept the increased risks of base jumping, and, having run a health system that served an area that attracted base jumpers to a bridge over a canyon, I can tell you that sometimes, things don’t end well for base jumpers.) But, even day-to-day, we make risk-benefit decisions. If you woke up this morning with a headache, you very well may have taken aspirin, acetaminophen, or ibuprofen for relief. Each of those medications carries certain risks (you might be surprised at all the risks listed for them), but for most, I doubt they gave that much thought, and merely wanted the headache to go away. Some people probably woke up to snow and ice on their sidewalks and the streets. You make a risk-benefit in deciding whether to shovel your sidewalk (as a physician, I can tell you that during these times, we see an increase in heart attacks and falls with injuries) and you make a risk-benefit decision in deciding whether to venture out on the streets, realizing that even if you are a highly skilled driver on the ice, in my experience, not an insignificant number of drivers are totally incompetent to drive on it.)
I also indicated that your risk tolerance may very well change at different points in your life. Those of us old enough likely remember well our “immortal years” of youth when we were game for almost anything and often failed to perceive or give proper consideration to risks that we wouldn’t dare take today, and we probably try to impart on our children that they should not take those same risks. I also took more risks when I was single than once I became married, both because of my increased responsibilities I felt I owed to my wife, but also because one of the reasons God gives us a wife is to tell us “no” when we come up with lame-brained ideas we want to try. For me, it became even more so once I had kids. I took fewer chances when I knew that if I became disabled or died, I would not be able to provide for them and they might have fewer opportunities. I purchased disability and life insurance to mitigate that risk. When I shoveled snow as a kid, I had no reservations. Now, I wait until it is light out, I wear more appropriate clothing and shoes, and I keep a phone with me in the event of a fall. Also, I am much more willing to accept the assistance of my grandkids to shovel the sidewalk for me!
So, let’s now put ourselves in the shoes of that 30-, 40-, or 50-year-old, married man or woman, with a family early in 2021. Faced with the information that there is a 75 percent chance they will be involved in an auto accident in the next year, how might they think about the risk? First, of course, there might be a few who would look at it as a 25 percent chance they won’t and not take any measures, thinking that chances are that even if they are in the 75 percent, it won’t be a big deal, certainly not worth changing anything in their lives or routines. On the other hand, I do think that most people’s self-assessment of their risk of being involved in an automobile accident in the next year is far less than 75 percent, in fact, I would think most people would put that risk at less than a percent. So, being told that their risk for that next year is 75 percent, I suspect that would grab more peoples’ attention and at least concern them initially.
Probably, a lot of folks would think, okay, that is a high-risk, but I can reduce that risk by not riding in a car with someone I don’t know to be a safe driver, being extra careful and taking an extra look before I cross streets, and when driving, I will be sure to wear my seatbelt and stay at or below the speed limit. If I go out to dinner or a party and have some drinks, I will make sure to have someone else drive or call a rideshare service. Those would all be reasonable things to do.
There might be others who might be even more concerned. For example, if that person is pregnant or the spouse is pregnant, that might cause some to assess the risks as even greater and to want to take even more precautions, e.g., returning home earlier in the evening to avoid driving in the dark and others who may have begun their evening partying and potentially be driving impaired. It might cause them to limit their driving on a holiday weekend or evening when it can be expected that more people will be on the road and an increased number of them might be impaired. It might cause the family to reconsider a planned road-trip for that year. It would likely cause them at least some pause about venturing out in the car on snow and ice or other bad weather, especially with the pregnant person and kids in the car.
There might also be some who realize that a parent, a disabled child, or other is dependent on them, and if they were to become seriously injured, it would directly impact that dependent person’s life and well-being. That might factor into their risk tolerance.
I think that the risk analysis for any novel virus causing an epidemic or pandemic is in many ways analogous. If I told you back in 2021 that your risk of getting infected in the next year was 75 percent, I think there would be many analogous thought processes. Unfortunately, due to misinformation and disinformation, I suspect many did not appreciate the potential risks of infection.
Just as with the risk of an automobile accident, there would be some people who would think, well, there is a 25 percent chance I won’t be infected, and even if I am, chances are it will be the “fender-bender” or someone backed into my car- type of infection, that is to say, “mild.”
I think that a fascinating way our minds work is that in both cases, we tend to focus on the immediate risks and not factor in, or give much weight to consideration of less immediate consequences. For example, in an automobile accident, we tend to focus on did the person survive and was the person able to walk away from the crash. However, there are a whole host of injuries that can occur. Some of those injuries can require surgeries to address, others can cause significant pain for a protracted period of time, others can result in disability, and some of these could impact our ability to work for a period of time or even indefinitely. And, of course, even if you are in an accident and not seriously hurt, it still could be that someone else in your car was hurt, someone in the other car was injured, or almost assuredly, a motorcyclist or pedestrian involved in the accident was seriously hurt. There can be traffic citations and court dates, criminal liability, lawsuits, and of course, the accident can result in increased future insurance premiums, especially if you were found at fault.
So, too, with COVID-19, the overwhelming focus by the CDC and by the public was on mortality rates, as if the outcomes of infection were either mild illness or you died. In actuality, there were many people who experienced protracted illness, including Long COVID, and these folks tended to be middle-aged – the very group that I used for our analogy above. There were others who developed cardiovascular complications of their illness and some of these people died months to a year or more following the apparent recovery from COVID-19 and these deaths were attributed to heart disease or stroke, and not to COVID-19. The key point being that when people evaluate their risk tolerance, they seldom factor in these longer-term risks and their consequences, which can lead to understating the risk of the accident or, for purposes of our analogy, the infection.
Further, we often focus our risk-benefit analysis too heavily on the impact to us individually, and not give the due consideration to the risk to others. As mentioned above, while we might survive the accident with no or only minor injuries, what about our spouse, what about our kids, what about others involved in the accident, and certainly motor vehicle accidents can pose risks to an unborn infant, even when the mother is not seriously injured. Similarly, while the infection of one person in the family may be mild, it can still cause severe disease in another family member who contracts the infection from that family member.
The point of all of this is to demonstrate that we humans are generally not good at conducting true risk-benefit analyses. It is for this reason that prior to the COVID-19 pandemic, public health and medical professionals most often recommended the “precautionary principle;” that is to say that until the risks can be better known, people would be well-advised to use precautions to avoid infection. But when we dislike the risk mitigation measures that would be necessary to reduce the risks, we are much more likely to rationalize and reduce the risks in our minds and to others. For driving, most people would likely have no problem with wearing seatbelts and recommitting to following speed limits. When told that we have a 75 percent chance of being involved in some kind of motor vehicle accident, we might even be willing to think that we would return home earlier at night, at least until we are with friends and really enjoying ourselves and not wanting to leave. We might even say we would put off a planned road trip until the following year, at least until friends invite us to go camping, fishing or rafting with them.
So, too, many took steps to minimize exposure to infection early in 2020. That became more difficult as society progressively returned more and more towards normal activities and ceased implementation of many of the protections that it adopted in the first year of the pandemic.
We heard many promoting on social media and cable networks that the vaccines were not safe, and this or that happened to some people who were vaccinated, which is surprisingly a very effective scare tactic and deterrent to immunization. However, every one of those doctors promoting these messages that I read or watched never presented the risks in a balanced way, as often what they raised alarm about occurred far more frequently and far more severely in people who became infected rather than through vaccination. It is impossible to make a personalized risk-benefit analysis when you are manipulated by unbalanced information. For example, I can tell you that almost any cancer drug is not “safe.” If I was seeing you in my office and only told you about all the terrible side effects and adverse effects you might incur with the chemotherapy, but did not indicate that there was any benefit in treating your cancer, of course no one would agree to undergo that therapy. If I only tell you the good about a treatment or only tell you the bad about a treatment, then I am manipulating you to try to get you to make a certain decision about your treatment. That is not informed consent. That is unethical to the foundation of medical principles.
To complete our analogy, it would not have been unreasonable to tell someone in 2021 that we could expect about a 75 percent chance that they would become infected with SARS-CoV-2 sometime in the following year if they were out and about as is typical – work, school, grocery shopping, social gatherings, etc. and they utilized no other mitigation measures. There were a range of mitigation strategies people could choose from that would decrease their chances of exposure and thereby infection. Once infected, for most of 2021, there was little we could do until you were at the point of needing hospitalization to reduce the severity of your disease and try to avoid death (an antiviral for outpatients did not get emergency use authorization until December of that year).
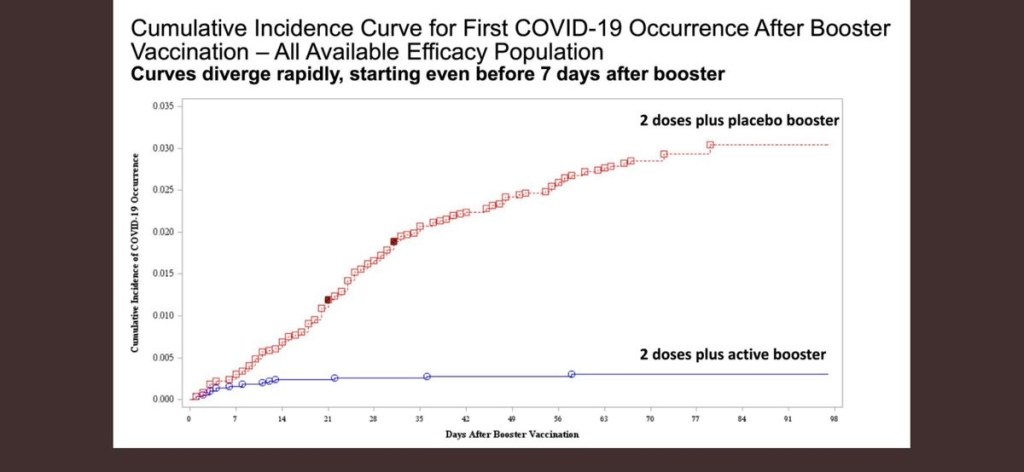
Vaccines were the game changer for reducing the risk of severe disease and death. During 2021, especially with the delta variant, the rates of hospitalization and death were many fold-reduced in those who were vaccinated versus those who were not. The problem is that we had no way to identify who would get severely ill if infected, just as in the analogy, I could not tell the person whether the motor vehicle accident (if they were part of the 75 percent) would result in hospitalization or their death. In both cases, it was the minority of all infections and the minority of all motor vehicle accidents. It is probably worth pondering that I have talked to a lot of people who unexpectedly got very ill from COVID or who developed Long COVID; almost none of them thought that would ever happen to them. Similarly, you may know of people who survived motor vehicle accidents or friends or coworkers who had a seriously injured family member or lost a family member to a motor vehicle accident. It is likely that none of them expected that to happen that day as the family member got into their car.
So, I will leave you with a framework for decision-making when we face the next pandemic with a new virus and you need to make the decision for yourself as to whether to take precautions to prevent getting infected for as long as you can or to buy-in to what will undoubtedly be people suggesting that large numbers of people need to go ahead and get infected to develop herd immunity or perhaps making the argument that it is good to get infected to build up your immunity:
- Look for trusted sources of information, e.g., the American Academy of Pediatrics, the American Society of Infectious Diseases, the American College of Physicians, CIDRAP (The Center for Infectious Diseases Research and Policy at the University of Minnesota).
- Be weary of doctors who don’t express uncertainty; don’t admit to having been wrong about anything; use political or inflammatory language when seemingly trying to educate the public; and aren’t willing to provide clinical studies to support their positions.
- If the novel organism belongs to the same family of viruses as ones we have experienced before, for example a coronavirus or an influenza virus, assume that the new virus transmits in the same ways as the known viruses do until proven otherwise. In other words, if there is an outbreak of a new coronavirus or influenza virus, assume that that there will be airborne transmission until proven otherwise and be skeptical of advice that recommends only washing your hands for infection prevention.
- Keep in mind that no virus that has caused a pandemic in the past has built up our immune system.
- Don’t buy in to any talk of herd immunity if you are hearing of reinfections occurring within a year.
- Remember that because vaccines use weakened, killed or only parts of the infectious virus, any adverse effect that you might experience with vaccination would likely be far worse with natural infection.
- Remember that your risk of more serious disease with infection with almost any organism will be greater if you have underlying health conditions, are immunocompromised, or are pregnant, and that the risk to the fetus is likely greatest in the first two trimesters.
- Finally, you would be wise to consider the precautionary principle. Use extra precautions until the disease outbreak has fully unfolded and you can see what kind of illness it is causing and how severe it is.