The problem in answering this question is that there are no precise definitions or criteria for determining whether a disease is endemic. But, generally, public health professionals refer to a disease being endemic when it is present throughout the year in relatively low and stable levels, and does not result in unexpected surges that would overwhelm health care capacity. The CDC defines endemic as “the constant presence of an agent or health condition within a given geographic area or population.”
I think it is helpful to better understand this by considering an example. I suspect that most all experts would agree that hepatitis C infection has been endemic in the U.S. since its identification and our ability to test for it in the early 1980s. To see this visually, let’s look at the epidemiologic curve “epi curve”) for hepatitis C. This is a graphic representation of the disease prevalence or disease transmission by plotting the number of cases along the ordinate (y-axis) and the progression over time on the abscissa (x-axis).
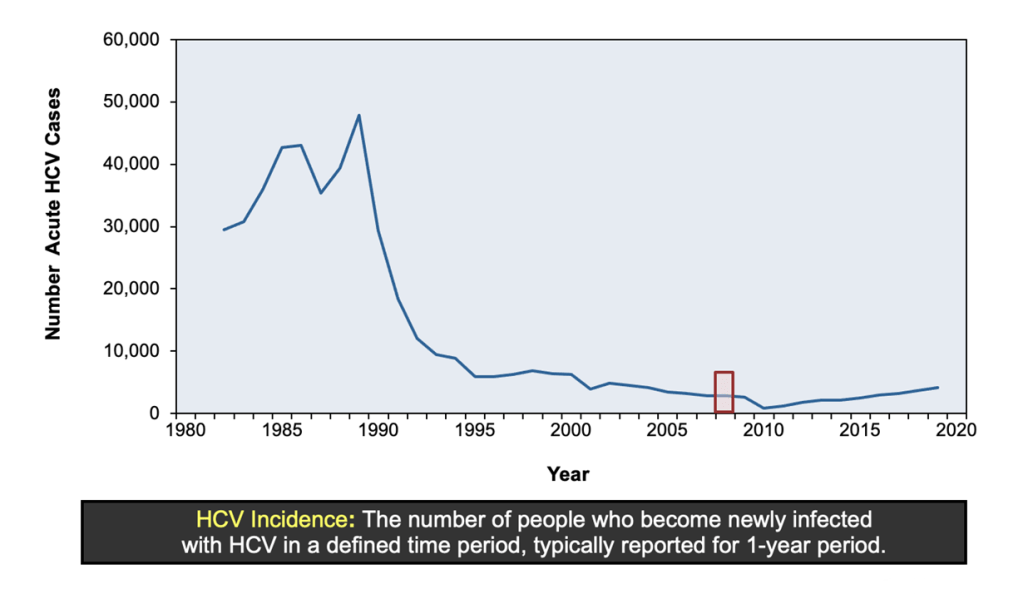
What you can see here is what would otherwise appear to be an unexpected outbreak or epidemic of hepatitis C over the decade of the 1980s. But, in reality, this was the result of testing the population for hepatitis C (screenings including blood donations and testing of those with liver disease) with newly developed testing and finding many people who had previously been infected. In other words, these were not all new infections.
Once we identified all of these previous infections, but continued testing, you see that from about 1995 on, we are identifying a relatively stable number of new infections every year. The epi curve from 1995 on gives us a typical graphic display of an endemic disease.
We can look at a different example – measles. Measles was quite common in the U.S. and is highly infectious, but an effective vaccine was developed and the U.S. made a concerted effort to eliminate measles from the U.S., which we did in 2000. That doesn’t mean that we don’t ever see measles cases, but these generally occur in people returning to the U.S. who are unvaccinated and infected in another country, or in groups of unvaccinated individuals when one of these travelers returns and is in contact with these unvaccinated individuals, often at school or in religious communities. Let’s look at Australia’s epi curve for measles.

The epi curve, reading left to right shows you the disease activity of measles in Australia prior to a national vaccination effort to control measles (Measles Control Campaign- MCC), then the disease activity during that campaign in the middle of the epi curve, and then the manifestation of measles as an endemic disease at the right of the curve following the campaign. Notice that when endemic, there still is some variation, but you no longer see the wide swings and surges that you see on the left hand portion of the epi curve.
So, now let’s look at the U.S. epi curve for COVID-19:

It should be immediately apparent to you that this is not representative of an endemic disease. This epi curve demonstrates a series of surges followed by low levels of disease transmission followed by more surges, and in fact, the most recent surge having been our largest yet. Another way to answer the question as to whether COVID-19 is now endemic is to ask whether the disease activity has (1) been predictable, (2) been relatively stable, and (3) has avoided overwhelming the health care system. I think the answer to all 3 would have to be no.
Well, if COVID-19 is not yet endemic, will it become so? I am not so sure. Remember the measles epi curve for Australia above and the development of an endemic following a vaccination campaign? Now, look at the U.S. COVID-19 epi curve and realize that we started our COVID-19 vaccination program in early 2021. Does it look like the pattern is evolving towards an endemic one? I don’t think so.
So, let’s look at the epi curve for another viral infection:
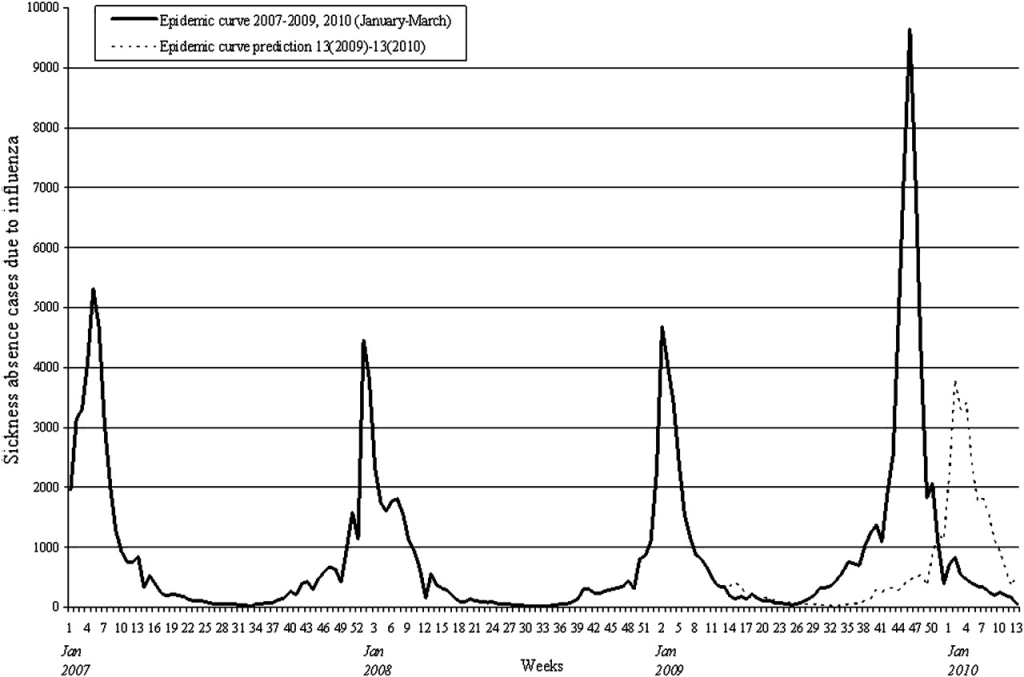
This is the epi curve for influenza from 2007 – 2010. Influenza is seasonal with fairly predictable times for outbreaks each year depending upon where in the world you live. Some people suggest the COVID-19 is also seasonal, but you can look back to the epi curve for COVID-19 above and see that it clearly is not. This influenza epi curve demonstrates an annual recurring epidemic. It returns each year and infects large numbers of people because that virus mutates frequently and not enough people get influenza vaccinations.
So, do you think that the COVID-19 epi curve looks more like (1) the U.S. hepatitis C epi curve and the Australian measles epic curve after the vaccination campaign, or (2) like the influenza epi curve? If you answered (1), then you would be in agreement with those talking heads that want you to believe COVID-19 is already endemic (though I would recommend an eye examination!). If you answered (2), then you understand why I disagree that COVID-19 is currently endemic. You may also now understand why I am not sure that it is headed towards being endemic, but rather I anticipate that it will be epidemic (like the influenza epi curve, though not seasonal) for the foreseeable future.
Of course COVID-19 might become endemic at some time in the future. It could be that a future variant might produce long-term natural immunity. It could be that much larger numbers of people will choose to get vaccinated. It could be that new vaccines will induce longer-term immunity. Lots of things could happen, but until something does, I don’t expect our epi curves over the next year or two to look like hepatitis C, but rather more like influenza, but with more frequent surges since COVID-19 is not seasonal (at least not at this time).

Dr. Pate, I’m so glad you don’t make this political, but so many people do, including doctors and scientists. I agree, this virus is not endemic (yet), but it will never be endemic until politics are taken out of the equation.
LikeLike
Yes, thank you! The politicization of this has cost so many people their lives and put so many at risk. That is one of my greatest regrets about this pandemic. Thanks for following the blog, Greg!
LikeLike
My friend, as long as you continue to blog, I will always follow it, been following it since you started early, guess it was around 2012 or so?
LikeLike
Wow! Yes, I think that is right! Thank you, Greg!
LikeLike
Excellent post! As the “other” Dr Pate and liver transplant doc, Hep C is now curable and rarely a threat to others. COVID-19 puts everyone at risk! We need to do our part. Lets help each other climb out of this! Its jyst a mask and one of many vaccines you have and will have. Lets get back to being us!
LikeLike
Thank you for your comment and thank you for following my blog!
LikeLike
Great explanation! Answers a lot of questions.
LikeLike
I so appreciate hearing your expert advice on a topic that has so much misinformation. I have an elementary age child with Celiac and Eosinophilic Esophagitis. He also has chronic abdominal pain we haven’t been able to manage yet. My kids have stayed in virtual school for the last two years to try to keep them safe. My family is up to date with our Covid vaccines. For a family with a child with chronic diseases, do you recommend we take a chance on in person school if no mitigation measures are used? I would appreciate any advice on how we can try to keep kids safe as we venture through this uncertain time…Thank you for all your efforts in spreading the facts!
LikeLike
Thank you for this question. It is a tough one. First of all, you are really helping your son by having everyone else in the household fully vaccinated and boosted. Studies have repeatedly shown that the risk is reduced for your child to be infected, no matter the variant, by everyone else being fully vaccinated and even more when boosted, even when the child is too young to be vaccinated or if the child’s immune response to the vaccine is reduced.
So, that is a great first step. The other step is to have your child fully vaccinated if he is 5 or older and sounds as though he likely is.
It pains me that your children have had to remain in virtual school because of the decision to not use other mitigation measures. I always want kids to be in school when it is safe to do so. I would suggest a visit with the principal. Have they employed mitigation measures you are not aware of, e.g., an increase in air exchanges per hour and/or HEPA air filtration if the air is recirculated? Are they supporting students in wearing masks if they wish to and taking a strong stance against bullying for it? How flexible would the school be willing to be to allow your child to attend in person when transmission rates are low, but to participate in on-line classes when transmission rates are high?
Then, a visit with your child’s gastroenterologist. Do any of your child’s medical conditions or the treatments being used for them create any degree of immunocompromise for your child? While I am not aware of any studies of COVID in patients with these specific medical conditions, are they? Is there any reason to believe that COVID-19 would be more severe in your son’s case because of his underlying medical conditions, that COVID-19 would aggravate his underlying medical conditions (we do know that the SARS-CoV-2 virus gets into the gut), or that your child would be at any increased risk for MIS-C or PASC?
As with most things, this is going to be a risk-benefit analysis, where you will have to weigh the risks of in-school attendance versus continued virtual school. However, I think that answers to the above questions and understanding how your physician assesses your son’s specific risks and what the school has done or is willing to do will help you in making this difficult decision.
What I can say is that your son is very fortunate to have such caring parents. Well done!
LikeLike