The CDC published their last Science Brief on the Community Use of Masks on December 6, 2021. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html. At that time the CDC recommended the use of masks to “prevent transmission of SARS-CoV-2” especially in light of asymptomatic and pre-symptomatic disease.
Here are the benefits of that strategy:
- Decreasing transmission decreases the potential for new variants of concern, which as we have seen have tended to become more transmissible with each new version and most recently developed some degree of immune escape/evasion, making protection from prior infection and vaccination less effective and making some of our therapies less effective or not effective at all.
- Decreasing transmission rates benefit those who are vulnerable (the elderly, those who are unable to be vaccinated, those with underlying medical conditions, the immunocompromised and those in institutional settings [nursing homes, prisons]) safer because the chance of encountering someone who is infected in their own families or when out in public is diminished.
- Decreasing transmission is also beneficial with a virus that is capable of causing long-term complications and disability.
Now, the CDC states that “community measures should focus on minimizing the impact of severe COVID-19 illness on health and society.” So immediately, you can see that the focus is no longer in preventing illness, but rather preventing severe illness. However, the strategy isn’t great for achieving that goal, because often the people who spread the infection to those who are at high risk for severe infection are those who are not themselves at high risk.
Dr. Walensky (Director of the CDC) stated, “This new framework moves beyond just looking at cases and test positivity to evaluate factors that reflect the severity of disease, including hospitalizations and hospital capacity, and helps to determine whether the level of COVID-19 and severe disease are low, medium, or high in a community.” In principle, I don’t disagree with this. I have always assessed multiple data points and different impacts as I have assessed Idaho’s or our local risk. The problem is the significant increase in disease transmission that the CDC is now willing to just accept (see below).
She also states, “This updated approach focuses on directing our prevention efforts toward protecting people at high risk of severe illness and preventing hospital and health care systems from being overwhelmed.” My problem with this statement is:
- It was a lot easier to identify those at high risk of severe disease back in 2020. Very typically it was people with advanced age and people with multiple medical conditions. We became much less able to identify these people as of last year as we saw more and more people in their 30s and 40s hospitalized, and often the only risk factor, if any, was being overweight. This kind of talk also resulted in pregnant moms not appreciating that they were now in the high risk group even though they were in their 20s and 30s, and we saw all kinds of disasterous outcomes for mom and baby. And, of course, since last year, we have gradually seen more and more children becoming ill and being hospitalized.
- This statement focuses on severe illness and preventing hospitalization. But, what about trying to prevent long COVID, MIS-C and many different long term complications that we are beginning to understand can result even from mild infection? I fear that we will see a significant rise in long-term medical conditions in those who have been infected, and likely especially those who have been multiply reinfected, along with the attendant decrease in employee productivity and increase in health care costs, which of course will then be reflected in everyone’s cost for health insurance.
- Again, the point I made above – one of the best ways to prevent people from developing severe disease and being hospitalized is to prevent mild infections in younger, lower risk. Why? If you look at infections in patients in nursing homes or inmates in prison, it was not fellow patients or inmates or visitors that infected them, it was the otherwise healthy workers who got infected and brought the infection in to the patients or inmates when they came to work. A lot of grandparents and other at-risk family members took many precautions with their every day activities, but they were infected by young family members who got infected at school or other healthy family members who got infected at work or gatherings and then infected the at-risk persons at home or during family gettogethers.
So, how big of a change is this guidance?
Here is our country’s risks levels immediately before the new guidance went into effect:

About 94% of the country was in areas that were high or substantial risk of disease transmission and advised to wear masks under the strategy of trying to prevent infections.
Here is the country’s risk levels immediately after the new guidance went into effect:

Wow! Now only about 30% of the country lives in areas of high transmission for which masks would be advised when the strategy is to accept a lot of infections, but try to limit overburdening of hospitals.
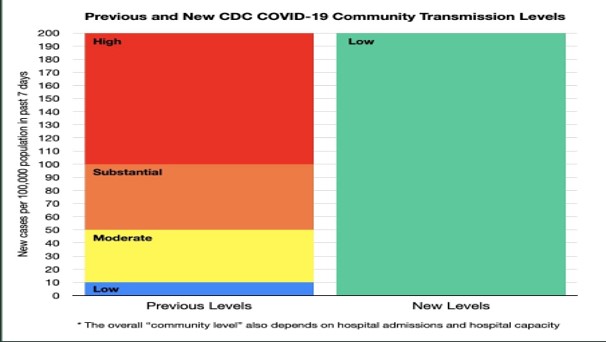
So, how did the risk levels fall so dramatically? The CDC accepted a higher level of disease transmission – up to 200 new cases in a week per 100,000 population. According to the CDC – the determination of COVID-19 Community Level begins by determining whether new cases per 100,000 in the past 7 days were < 200 or > 200. (For those who, like me, like to follow the 7-day moving average of daily new cases, this cut-off at 200 roughly translates to 28.6, which has generally been associated with accelerated community spread.)
One of the reasons for the CDC allowing higher transmission is that we now have more testing and therapeutics. That is true now that cases have come down so much, but ask anyone who tried to find at-home tests a month ago how easy that was and ask anyone who got sick with omicron who was at higher risk whether they were able to find an infusion center that was able to administer monoclonal antibodies or a pharmacy that had stocks of antivirals. I tried to help a number of people in Idaho and in Texas who got ill and was unsuccessful in all but one case (and, even then, I spent hours on the internet and on the phone trying to locate the treatments). What assurance do we have that we will have plenty of therapies with the next surge, assuming that the next variant is still susceptible to these treatments?
Another reason the CDC suggests as to why it can tolerate many more infections is the “high rate” of vaccination in the U.S. Really? We have 65% of the population fully vaccinated and there have been many countries with far higher levels of vaccination who have had huge surges and large numbers of hospitalizations in the past few months.
So, here are a couple of graphs that will help illustrate what a dramatic shift the CDC is making:
This next graph (an epi curve) will show you how this masking guidance would have played out had it been in effect for the entire pandemic with the surges the U.S. went through.

Here is how one social scientist paraphrased what the CDC’s new guidance was in essence stating: “It’s safe for you to take off your mask because when you get (COVID-19) there is still plenty of room at the hospital.”
I understand the loss of patience for masking by the general public. However, I fear that it is because we haven’t done a good job of educating the public that bad stuff can still happen even if you survive the infection. I talk to a number of these patients. That is why, along with the fact that I want to protect babies, toddlers, grandparents and the immunocompromised, I will be sticking to the old guidance for my own personal masking decision.

Thank you Dr. Pate, for this thorough review of the CDC’s latest position and guidance. You have validated all the concerns I have been having about this change in the CDC’s guidance. I wonder how much of the CDC’s changed position regarding masking is in reality a political move, or perhaps a short sighted effort to balance public health with economic factors, which I do not believe is the CDC’s responsibility.
LikeLike
Hi Dr. Pate – Thanks so much for sharing your thoughtful analysis and reasoning for continuing mask use. It is an extraordinarily complex time as the infection rates and other metrics move in positive directions, and different experts come to sometimes contradictory conclusions about what the appropriate actions might be and when (or if) to modify masking and other behaviors. I wonder: what circumstances would need to exist for you to feel comfortable changing your masking recommendations? Or, will masking need to be a permanent part of our existence if COVID becomes endemic (since vulnerable populations like babies, toddlers, grandparents and the immunocompromised will always be part of our community)?
LikeLike
Hi CJ,
Great question. Certainly, once we get to COVID being endemic (which despite what you are likely hearing, we are not there yet – in fact, I will be posting another blog piece about what endemic means and what it looks like very soon), then I will not be masking except in very limited circumstances. But even before that point, if I am not seeing worrisome variants on the rise and if our weekly case rates are down to 10 cases per 100,000 or less, then I likely won’t wear a mask most places. What I would have liked to see from the CDC guidance was consideration of a combination of factors (these are the ones I have used) – disease transmission rates, variant of concern activity, and vaccine effectiveness.
Thanks for your question and thanks for following the blog.
LikeLike
Hi Dr. Pate,
Thank you for the information. I’m a bit confused about what is considered safe at this point. Would it be considered safe for a person to wear a good mask and ride a charter bus for two and a half hours even if the others are not masked? The person is an obese male, over 55 with diabetes, he’s had 3 Pfizer vaccines. How at risk would this put him? His work is requiring this travel to and from a large business conference at a hotel. It sounds very risky to me but perhaps I am being too conservative. I’d appreciate your input.
Thanks,
Karen
LikeLike
Hi Karen,
That is a tough question. It is indeed confusing. So, here is how I think through these various scenarios people give me.
1. First, I examine the risk of the specific person. So, his age puts him at more risk that the average adult, but not in the very high risk groups of >65 and even higher risk group of those >75. On the other hand, his obesity and diabetes place him at even greater risk than someone his age without those factors.
2. Then I look at the mitigations the person has taken or is willing to take. He is fully vaccinated including a booster, so that is his greatest protection against getting severely ill or dying if he does become infected. Also, you indicate that he is willing to wear a “good” mask (I would recommend a N95 if he is able to wear it comfortably) and that will further reduce his risk, if he wears it correctly and consistently.
3. Then I look at the risks posed by others and the specific activity. In this case, he will be on a charter bus for 2 1/2 hours. That is a very long time and big concern if (a) there will be a lot of other people on the bus; (b) he does not know the other people on the bus and what precautions they have taken or will be taking in their own lives to reduce the potential of being infected; (c) if the bus recirculates the air in the bus (my guess would be it does); and (d) if the air is not filtered (e.g., MERV13 grade filter, and I very much doubt the bus would have that) and there are not many air exchanges per hour (e.g., only 2 – 4 exchanges per hour). One way for him to get an idea of how good the ventilation is on the bus is to take a CO2 monitor on the bus and see how it registers. Another way to improve the ventilation is for him to sit by a window and open the window if they allow that. If they do not allow that, then if he has any vents above his head or in the area of where he is sitting, have him turn them on as open as they will go.
4. Then, finally, I look at the situational risk. What variant is circulating and what is the disease transmission level where he is travelling to and from. Don’t use the current CDC new levels for this as they will paint the picture as much better than it is. The higher the disease transmission rates where the other people on the bus are coming from, the higher the risk someone on the bus may be infected and not know it, and you indicated that they likely won’t be wearing masks, which means that infectious virus, if any, can be circulating throughout the bus (not just 6 feet) on the airstreams, which is why I focused on the ventilation and air handling. I am most worried when the disease transmission rates are more than 10 daily new cases per 100,000 people and least concerned when it is <1.
Finally, we have the issue that we are currently evaluating the extent of the waning of immunity from the booster shots. It is clear that if his booster was within the past two months, he should be in good shape. If it was much longer, we are less sure especially in the face of omicron and the new variant BA.2 that we are watching closely because it is rising in prevalence and concerned that we may see a surge in the next 3 – 6 weeks. BA.2 has the ability to partially evade the immunity of prior vaccination or infection and is even more transmissible and I would not want to be in any indoor setting (including a bus) with a lot of people who I don't know and who are not wearing masks if we do begin to see a surge with BA.2.
That was a lot, but I hope that helps.
LikeLiked by 1 person