I am beginning my blog series on what is known about the medical and health consequences of COVID-19. Before jumping in, I indicated that readers would need two tutorials in preparation. The first we covered in the last blog piece. That covered different types of clinical trials and a brief tutorial on the statistics that we use to interpret the results of clinical studies.
Today, we will complete the other tutorial – a basic understanding of virology and immunology, one that is so brief and basic that it is sure to offend microbiologists, virologists and immunologists, because in being so basic, there is much that we won’t cover and do justice to, but also, we won’t be able to cover all the intricacies and the exceptions to general principles that a non-scientist will not need to know in order to gain an understanding of the health effects from infection with the SARS-CoV-2 virus.
So, let’s take on virology first. Let me first confess and let you know that in explaining viruses, I will do two things that are wrong, but I don’t know a better way to help non-scientists understand viruses. First, I will lead you to believe that viruses are living things. They are not. I will write things that discuss “killing” the virus, which would lead one to believe then, prior to killing, they must have been alive. It probably would be better for me to be more precise by stating that the virus is “inactivated” or “altered” to render it no longer capable of infecting a cell, but I find it a lot easier to just say the virus is killed, even though that is not technically correct. I am also in good company, because most of the virologists and microbiologists I talk to also use this phraseology, even though they know this is not technically correct. In fact, we even refer to “live” virus and “killed” virus vaccines as a simplistic reference to whether the vaccine can or cannot cause infection. (By the way, we do not use “live” vaccines for prevention of COVID-19).
The other thing I will do is give you the impression that viruses are intentional beings, which they are not. It is common when we discuss how viruses evolve to use language that suggests the virus is getting smarter and craftier, with the impression that the virus is purposefully trying to preserve its ability to transmit and infect its host. Certainly, we do see many viruses evolve in this manner, but there is no mind, consciousness or intent with respect to viruses. Again, it simply is a bit easier to understand and converse about these evolutionary changes by thinking about what is best for the virus and how it might choose to act if it could do so, because obviously, if a virus doesn’t evolve in a manner that preserves its ability to transmit and infect, then it is not going to pose much of a threat to us and we are not going to spend a lot of time worrying about those viruses.
With my confessions out of the way, we can begin. What is a virus? There are a number of ways we can divide viruses up into categories -the size of the virus, plant vs. animal viruses, human vs. non-human viruses, the family of viruses to which it belongs (e.g., coronaviruses), whether the virus has an envelope or not (SARS-CoV-2 does) and a number of other ways, but one common way is to divide them up according to the make-up of their genetic material – DNA viruses and RNA viruses. SARS-CoV-2 is an RNA virus. DNA and RNA contain the genetic instructions for the production of protein and new viruses. But, having the genetic code is not enough, and this is a big problem for viruses. (You may be wondering what does it matter whether a virus is a DNA virus or an RNA virus. The majority of examples of viruses that have a latent phase in humans, i.e., you get infected, but then the virus can hide out relatively dormant until manifesting itself years later are DNA viruses. As we will see, SARS-CoV-2 may be one of the exceptions to this rule. RNA viruses generally undergo much more rapid replication and often do not have the mechanisms that help prevent errors or repair these mistakes in the replication process. This leads to mutations, which can change the properties of the virus and may make antibodies formed to the version of the virus prior to the mutations less effective (immune escape or evasion). We have seen many examples of this with the SARS-CoV-2.)
Viruses need the machinery contained within a cell to make the proteins and to assemble all the pieces of newly reproduced viral particles into virus progeny. In other words, viruses can only replicate when they infect a cell so that they can take over the cell’s machinery. If a virus is airborne or on a surface like a countertop, it may or may not be able to infect a cell if it comes into contact with a host, but it is not replicating while in the air or on the surface. When the virus does infect a cell, instead of the cell’s machinery making proteins coded for by the cell’s DNA, the cell is now hijacked to use the virus’ genetic material to make the proteins needed to assemble new viruses. The virus has two more challenges, though.
First, if our immune systems are working properly, they are not going to welcome the virus into the body. As soon as our bodies recognize an invader, our immune systems launch an attack. From the time the virus enters our nose, mouth, lungs, gastrointestinal tract or blood until the time that it can invade a cell, it is particularly vulnerable to this attack. We’ll talk a lot more about this when we get to the immunology primer below, but keep in mind that before the virus enters a cell, antibodies can attack it. Once inside the cell, antibodies can’t get to the virus. (Keep in mind that there are millions of Americans who have immune deficiencies or states of immunocompromise where various portions of the immune system may not work well or work at all. For example, there are conditions where people don’t make certain antibodies or any antibodies. Also, many people have underlying health conditions for which the treatment has the effect of weakening the immune response. These folks can all be much more susceptible to infection than the rest of us, and if they get infected, they may be unable to clear the virus on their own.)
The second challenge for the virus is that it can’t just invade any old cell it wants to (see how I make it sound like viruses have minds and intentions!). Just like when we check into a hotel, we will get a room key that works just on one door and allows us to enter one room, the virus can only enter and infect cells that it has a “key” for, but in this case, we refer to the lock on the door as a receptor on a cell surface. With SARS-CoV-2, this is why you have heard so much about the ACE-2 receptor. This is the door lock to the cell for which the SARS-CoV-2 spike protein (specifically, something called the receptor binding domain or RBD) serves as the key. Now, this is where my analogy falls apart because unlike the single hotel room for our key, there are many, many cells that have the ACE-2 receptor, and thus they may all possibly be vulnerable to infection. In fact, this is in large part why we see so many different possible manifestations of SARS-CoV-2 infection.
The other way my analogy fails is that the SARS-CoV-2 virus also has a trick up its sleeve (see again how I am giving you the impression that the virus is alive, cognizant and tricky!) in that it has an alternative way into cells, kind of like if we forgot the key to our house, we might still be able to get in through an unlocked window. Nevertheless, knowing that the receptor for SARS-CoV-2 is the ACE-2 receptor and knowing which cells have ACE-2 receptors on their surface will help us a lot to understand all the ways the SARS-CoV-2 virus can wreak havoc on our bodies and why we see so many different manifestations of COVID-19 among people who get infected.

Above is a depiction of the SARS-CoV2 virus. First notice the red projections. These are the spike proteins that are able to bind to the ACE-2 receptor on cells that the virus can infect. This is the protein that the mRNA in the Pfizer and Moderna vaccines code for. That means that you can receive the genetic instructions that tell your cells to make the spike protein (but no other parts of the virus, so no infection can result), but your body will recognize the spike protein as an invader and form antibodies against it that will be at the ready should you be exposed and infected by the actual SARS-CoV-2 virus. Remember from above that the antibodies can only stop the virus before it enters the cell, so having premade antibodies (a process that can take 5 – 10 days) is a real advantage in fighting the virus and preventing significant infection.
There are other proteins besides the S or spike protein, including the E, M and N proteins. You will recall from above that I indicated that the SARS-CoV-2 virus has an envelope (not all viruses do). An envelope is the outermost layer of the virus and it serves to help protect the virus’ genetic material. The E protein is part of that envelope. The M protein is associated with the virus membrane. The N protein relates to the nucleocapsid.
So, a person who has been infected with the virus will often have antibodies against most or all of these proteins, whereas someone who has been vaccinated, but not infected, will only have antibodies to the spike protein, since there is no viral membrane, envelope or nucleocapsid in the vaccines approved for use in the U.S.
So, here is a look at the SARS-CoV-2 virus in a clinical specimen from the first patient known to be infected in the U.S. using a special kind of electron microscope and a stain that turns the virus particles blue. The virus particles are the blue circles, most of which are inside cells that they are infecting:
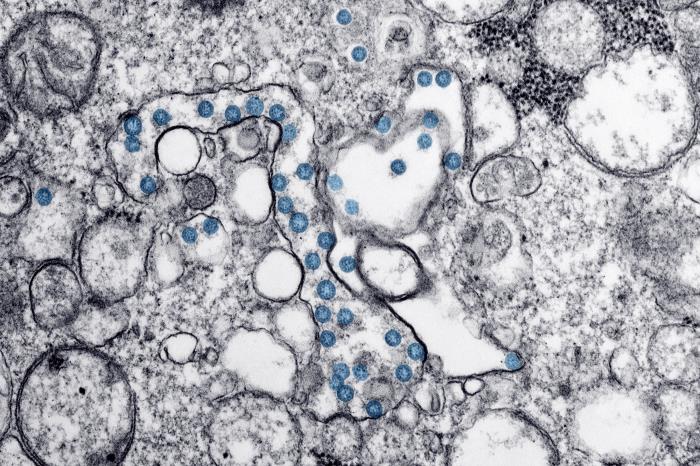
In this case, the viruses that are inside of cells would no longer be susceptible to antibodies.
Here is another image from the same patient. In this case, the virus is not stained blue, but you can see them as the small black circles. But, notice that most of these have not yet entered a cell to infect the cell:
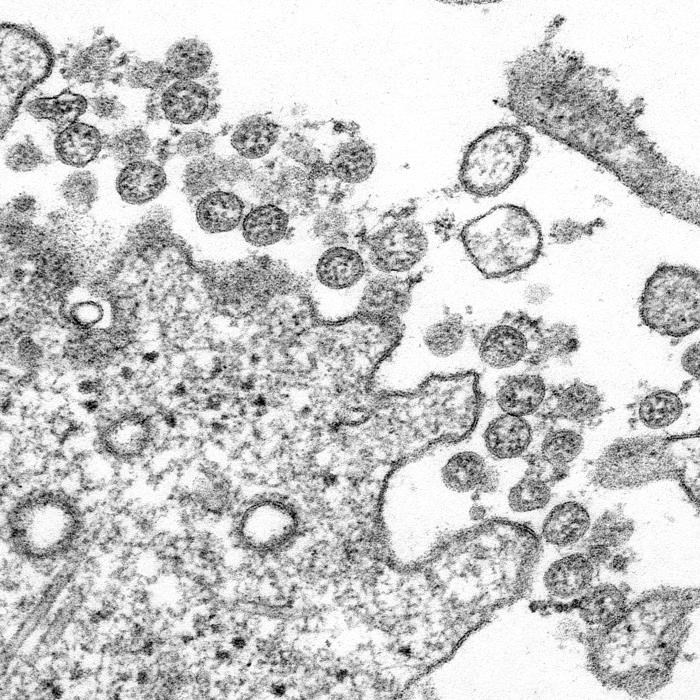
In this case, antibodies can bind to the virus and when those antibodies are effective in preventing the virus particle from entering a cell, we call those neutralizing antibodies. Not all antibodies are neutralizing; some bind to the virus, but don’t block the virus’ entry into the cell. That doesn’t mean that those antibodies don’t sill serve a purpose, but they may not be enough to prevent infection of cells.
Okay, just a little bit more and we will move on to the immunology tutorial. We will refer to viral load which is a reference to how many virus particles are in your nose or throat or wherever we are measuring it. But, what we are often more interested in is “infectious” viral load, something much more difficult to measure, but an indicator of not just how many viruses are present, but how many of those virus particles are infectious to someone else. Remember that if you are normal, you will begin attacking the viruses in your nose, throat, lungs, etc., so some of those viruses are rendered incapable of infecting someone else, and while they would be detected as part of the viral load, they would not be part of the infectious viral load.
Conversely, we talk about viral dose when we try to quantify how many viruses do you have to get in your nose or throat or lungs to cause infection or what amount were you exposed to. Oftentimes, being exposed to a higher amount of virus can produce more severe disease. This is where masks come in and the public has missed some of the nuance here. Masks don’t have to filter out every virus particle in order to help protect you. If they filter out enough of a virus, it may mean that you are exposed to so few virus particles that you do not become infected (although for SARS-CoV-2, a recent study shows that it doesn’t take many virus particles to cause infection), but even if you do get infected, having blocked a lot of the virus so that you received a low dose may make it more likely that you will only have a mild or moderate infection.
Now for a bit of immunology.
The immune system is actually very complex. Most often, people equate antibodies with immunity to something, but antibodies are just one part of a very complicated system, and having antibodies to something doesn’t always mean you are immune to it. I had a teacher ask me to explain the immune system as if I was teaching one of her 5th grade students. That is not easy to do, but here is some of what we know about the immune response to SARS-CoV-2 for a 5th or 6th grader:
If a bacteria or virus invades your body, and you have never been exposed to that invader before, the first response of your body is to send in ground troops that will try to stop these invaders at your border (your skin or just under your skin if you get cut, or your nose and throat if it is trying to invade your body there, or your gut, if it is trying to make entry there).
The ground troops with their rifles are called white blood cells (or white cells, but not all white cells. We are going to talk about other white cells that are critical, but aren’t major players in this initial (innate) immune response later), and they don’t care who the enemy is, they just attack and try to shoot anyone (in this case a bacteria or virus) who doesn’t have the same uniform as the rest of the body (in this case, features that these white cells recognize as being your own body as opposed to an invader).
Just like we have different military forces (Army, Marines, Navy, Air Force, Coast Guard, National Guard, etc.), so too these white blood cells all have slightly different roles and tactics to attack an enemy. We have many different types of white cells in our blood, and they each conduct different kinds of warfare against these bacteria and viruses.
Just like our ground troops can throw a hand grenade or fire a cannon and blow up our enemies as well as things around them that we might otherwise not want blown up (like innocent bystanders or buildings, etc.), our white cells start releasing chemical warfare (chemokines, cytokines, etc.) against these invaders of our bodies and they cause some indiscriminate inflammation and surrounding tissue damage, as well, but as an attempt to kill these invaders or at least slow them down (if you got a cut in the past that got infected, you saw the redness and swelling that resulted, which is a result of this process).
What our ground troops (white cells) are trying to do is prevent these invaders, in this case a virus, from crossing that boarder (our nasal passages and throat in the case of SARS-CoV-2) and entering into our towns and cities (in this case our cells), where they can take over our food supplies and manufacturing plants that will allow them to make more invaders (viruses) that can then increase their attack on us.
This chemical attack is what makes us feel bad – fever, aches, cough, runny nose, etc.
Now, all this time that our ground troops (white cells) are fighting the invaders (virus) off at our borders with their rifles, hand grenades and cannons, they have already sent the message back to headquarters that we have invaders, a sample of what they look like, and a request that we need some weapons that will specifically target these invaders to stop them before they get into our towns and cities (cells) where they will make more invaders (virus). These weapons will be very specifically targeted to this invader (think like drones and laser-directed missiles) so that they only kill the invader and don’t cause all the collateral damage (destruction of property and injury or death to our own body’s cells and tissues as friendly fire, although like a drone, sometimes we target something we think is the enemy, but is not. In the case of our antibodies, this can mean that a part of our body becomes the target of the antibodies and this can result in auto-immune disease and we refer to those antibodies as autoantibodies).
HQ then revs up the manufacturing plant and starts making these highly targeted bombs (antibodies) that recognize something that is different that makes up these invaders that is not present in our normal body cells and tissues. This different thing is called an antigen and HQ manufactures these special bombs (antibodies) that only blow up anything that has that particular antigen and leaves everything else alone. It ordinarily takes HQ 5-14 days to make these specialized bombs (antibodies).
In the meantime, our ground troops (white cells) have to hold off the invaders. Sometimes they do, but often times, some of the invaders get into our towns and take over the food supply and start manufacturing new viruses.
Now, if you get an antibody test while you are sick (in this case, COVID-19), but before HQ has had time to make antibodies, the test will be negative, even though you are infected. This is called a false negative. It is also possible that you had some left-over antibodies from a prior invasion (COVID-19 infection), but you already defeated that invader, and perhaps now when the antibody test is measured, you were suffering from a cold virus or influenza virus. This positive test for SARS-CoV-2 antibodies would not indicate that you have acute SARS-CoV-2 virus infection at this particular time.
Now, these bombs (antibodies) come in a number of different kinds. Antibodies do often defeat invaders, but not always. We have examples of other virus invaders where HQ makes plenty of antibodies, but the invaders march on and take over our cities and don’t seem to be slowed down by the antibodies. In the case of this coronavirus, we think antibodies are important, but they are not the only thing that is important, and we still do not know how many antibodies you need to be protected from infection, which kinds of antibodies are needed, and if you have them, how long they will protect you.
Now, back to the types of bombs (antibodies). It turns out that you need one kind of antibody if the invader is crossing the skin (IgG) and you likely need a different antibody (IgA) if the invader is crossing a mucosal border (your nose or gut). Polio was a gut invader. We developed two different vaccines – a shot and a sugar cube, and it turned out that the sugar cube worked the best, because it caused HQ to make IgA better than the shot did. Everyone talks about IgG and that is what the COVID-19 antibody tests check for (much less commonly tests will include IgM levels), but it may be that IgA is very important in preventing SARS-CoV-2 – we don’t know (or at least I don’t). The good news is that in one of the first vaccine trials to be reported, it appears that the vaccine does stimulate a robust response of both IgG and IgA.
Okay, back to the types of bombs HQ is making. In addition to different types of antibodies like IgG and IgA (and there are others), some of these bombs are really powerful killer bombs called neutralizing antibodies, because in a test tube, they keep the enemy from entering into our towns and cities (cells), and if the invaders can’t get into our cells, they can’t make more invaders, so, when we shoot or bomb all of the invaders at our borders, its over because there are no more invaders.
Let me add that we don’t know that an antibody is truly a neutralizing antibody in someone’s body just because it is in a test tube, but in the case of the SARS-CoV-2, it does appear that these neutralizing antibodies are very important in our protection and that they do tend to be effective, though we saw that with omicron, these antibodies were less neutralizing than with prior variants. So, while neutralizing antibodies do seem to be important in the immune response to SARS-CoV-2 (this was not a given because there are other examples of viruses that induce lots of neutralizing antibodies to be produced, yet they don’t slow or stop the infection), other antibodies that bind to parts of the virus but don’t prevent cell entry (called binding antibodies) also seem to play an important role in our defense against SARS-CoV-2. It turns out that some of these other bombs (binding antibodies) are like paint balls/pellets, where you shoot the invader and it doesn’t kill them, but they are now marked. Marking these invaders can help other parts of our immune system go after them. This other part of the immune system is called the cellular immune system.
In this case, HQ is not only making highly specific bombs (antibodies – for extra credit, this part of the immune system is called humoral immunity and for credit to skip a grade, that part of the immune system with our troops on the ground at our borders is called innate immunity. It is innate because we are born with it and it does not require ever having been exposed to something to fight it. It is ready to fire on sight), but also plays a key role in messaging to HQ that we need to make highly specialized tanks (T-cells).
Remember, the humoral immunity – antibodies – takes time if you have never been exposed to that invader before. We have to get the body part to HQ, HQ has to design a blueprint for the bombs, and then we have to manufacture the bombs (antibodies) and that all takes about 5 – 14 days.
While HQ is mass producing bombs (antibodies), they have also been producing highly specialized tanks (T-cells – part of what we call cellular immunity).
These specialized tanks (T-cells) also come in several types. As, I mentioned previously, the goal of our innate immune system (our troops at the border) is to kill the invaders, or at least hold the invaders from getting to our towns and cities (our cells, where they can take over our manufacturing plants and make more invaders) until HQ has time to produce the specialized bombs (antibodies). Once an invader gets into a city, our innate immune system is not very effective and our specialized bombs (antibodies) generally can’t get inside to capture the invaders. It’s like ISIS getting into a town or city where they can create a stronghold and many barriers of protection as opposed to being out in the open in the unoccupied land by our borders.
So, HQ makes these T-cell tanks while they are making the antibodies. One of these tanks has the ability to find pieces of the invaders and it amplifies the attack in those areas (helper T-cells). Another type of tank can identify which towns or cities (our cells) have been invaded, and while our antibodies can’t penetrate the invader’s hold on the towns, these tanks just blow up the cell and kills all the invaders who are occupying the town (our cells) (these are called cytotoxic or killer T-cells – in the studies we are going to look at, these will often be referred to as CD8+ cells reflecting that we can identify these specific cells based on them having the CD8 marker on them). And, thinking ahead, HQ makes tanks with advanced radar, infrared detection capabilities and other abilities to quickly detect these same invaders again should they ever try to cross our border again once we have defeated them (memory T-cells – these are often referred to as CD4+ T-cells because they are positive for this marker). The long-lasting antibodies and the helper and memory T-cells are useful, because while the first time we face an invader, the entire range of our arsenal (humoral- antibodies- and cellular – T-cells) takes 5 – 14 days to mount our full response, the next time we see the invader, all of these parts of our immune response can be called to duty almost immediately, so much so, that we often will not get sick or have any symptoms, or if we do, with some unusual exceptions (like Dengue fever- due to a phenomenon called antibody-dependent enhancement or ADE, something you may have heard about early in 2020 when we feared this might also be the case with SARS-CoV-2, but we were relieved to find does not happen contrary to some doctors who still suggest it does in their disinformation campaigns), we will only have a mild case.
What we also found out is that while the antibody response to SARS-Co-V-2 infection is not always robust or long-lasting, the cellular response in nearly everyone was. Not only did those who did not mount a very good antibody response develop a good cellular response, but even family members who lived with someone who was infected, but to the best of our knowledge, did not get infected themselves, still developed a good cellular immune response! And, for many viruses, we know that the cellular immune response tends to be more important for viruses, because there are diseases that you don’t produce antibodies, and these patients tend to get serious bacterial infections, but not severe viral illnesses; while there are other diseases for which patients have problems with their T-cells and they tend to get bad and prolonged viral infections, like shingles that will occur in multiple locations (whereas shingles tends to occur only in a single area in those with otherwise healthy immune systems). COVID-19 appears to be a disease for which both the humoral (antibody) and cellular (T-cells) responses are important.
Vaccines can often be engineered to trigger specific antibody responses that we want (like neutralizing antibodies against a specific part of the virus that appear to be especially protective against viruses getting into cells), but they also often trigger the cellular immune response. Even if the antibody response declines over a few months, we have many examples (e.g., measles) where the memory cells specific for that virus can persist for many decades, if not the remainder of your life. With COVID-19, the immune response thus far, to the currently available vaccines, does not appear to be long-lasting (certainly not life-time), but it does appear that the cellular immune protection may outlast the humoral (antibody) immune response, which may explain why, over time, we may be more prone to breakthrough infections (if previously vaccinated) or reinfections (if previously infected), but yet don’t seem to be as likely to become severely ill. However, as you will see, recent studies are showing that some people who get infected are developing immune disturbances that can result in those people having more severe disease with reinfection, despite the common misinformation that infections build up your immune system. We have to remember that the immune system is a delicate balance between many different chemicals, antibodies and cells that can all work together in the right balance to protect us, but call also easily become out of balance and actually cause harm in an uncontrolled and overly exuberant response which appears to be playing a role in why certain children develop MIS-C (Multisystem Inflammatory Syndrome – Children) and certain adults develop critical illness with manifestations of cytokine storm.
I think this is enough for now. In my next post, we will dig into what health effects we are seeing in those who survive COVID-19.

Dr Pate,
Great article.
Thank you
Sincerely,
Michael Haley
LikeLike
Thanks, Michael. We’ll start digging in to what we know about Long COVID and other long-term health consequences resulting from COVID-19 with the next blog post. Thanks for following the blog!
LikeLike
>
LikeLike
Excellent! It may take a couple of read throughs but the information is great!
LikeLike
Thanks, John. Yes, this is complicated stuff. I have done my best to make what is very complicated as simplified as possible, but I still learn more every day. But, as we go through this blog series, I will try to apply this introductory material to the facts of how this is playing out in human patients as we proceed and that may help make a lot of this more clear, as well. Thanks for following my blog and stick with me. I think more will become clear as we get into this. Of course, the thing is, as you learn more, you better realize what we still don’t know!
LikeLike
Great, Quality Content, A lot of thanks for sharing, kindly keep with continue !!
LikeLiked by 1 person
Thank you, Pramod!
LikeLike